I’ve a couple of blogs whirling around my mind now, and knowing what to say and when to say it is often the thing that stops them from moving from my brain onto the paper (well virtual paper). I’m also a little unsure who would want to read too, but Coach Sharon says, ‘just put it out there and see what reaction you get’.
This week started off a bit challenging, as well as my main job at Redmoor Health, I still work in General Practice, and I was onsite at the surgery for the day. I had 3 tasks that have been niggling for a while, but I found each one so convoluted, I didn’t fully complete any of them. I was despondent and also fully understanding of why change in the NHS is flipping hard and takes time. So, I’ve decided to work backwards in sharing this week, as it most definitely ended on a high.
I’ve been lucky to go to Camp Digital for the last few years, hosted by Nexer Digital and as ever the speakers and people who attend inspire, uplift and confirm my hope that the start of my week’s challenges can be resolved with the right approach. There is a community of wonderful people, passionate about making things better, focussed on user research and digital transformation truly grounded in data, design, and experience. I hope some of them move into or stay in the NHS and not leave it, I hope others move to product suppliers and service design to build things better from the start. I also hope they have the opportunity and confidence to speak up and say, ‘this is too early to ship to market, we have more work to do’.
Having been in the workplace for 40 years this month, ‘improving’ is as much in my nature as is ‘sharing’. Work started for me in the nuclear industry with Quality Control, then Quality Assurance in 1983 and 1991, moving into the NHS 20 years ago with a stint in Service Improvement, then Commissioning and provision in General Practice. So James Plunkett’s keynote session was easy to relate to. James weaved his story of ‘history rhyming rather than repeating’ through the opportunity for scaling up and consistency, via Ford’s mass production, to making beautiful artisan loafs into the mass produced, square, white stodgy thing that many may think of as bread today. James absolutely recognised and rubber stamped the mantra that digital transformation is ‘all about the people and ways of working’, not just the tech. This is one of my favourite T-shirt slogans. Watching the NHS attempting to scale up, deliver consistency and increasing its awareness of quality improvement right now, feels like we are at a junction where we can go down the path of mass production, using methodologies and run charts, or, we can pause, and have QI in our minds as we ask curious questions to understand ‘what is the problem we are trying to solve?’, who’s involved, what are the issues, and then assess which approach can help. I’m minded to use the term ‘optimise’ a little less often now though James, but I loved this slide.
In the second keynote, Shabira Papain of People Street, shared her fun, obvious passion, and practical advice to explore social justice, and design for the 20% who are most likely to be digitally excluded. The NHS catchily refer to elements of this as Core20PLUS5.
Sketchnote by @ChrisSpalton
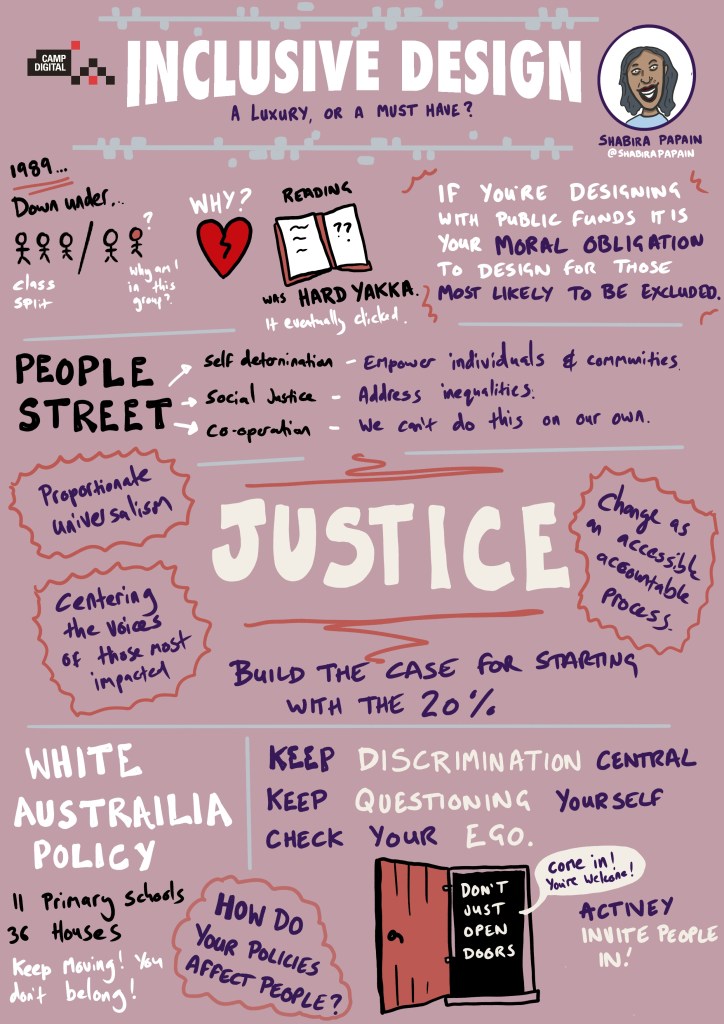
As public sector workers, we were challenged with the moral obligation to design for those who are excluded and not just to ‘open doors’ but to ‘invite people in’. This reminded me of earlier in the week, as I had just added ‘Register with a GP Surgery’ to our practice website, to help new patients register online instead of having to come into the practice and fill in a form (currently comprising 12 sides of A4 paper). Then our practice manager instinctively went a step further, got an iPad out of the cupboard (that’s another story), loaded up the site and showed the Receptionists how to help people who may be excluded from this new process, either because they don’t have devices, data or confidence to do this. Now, someone in the team can sit with people who need help to fill it in, rather than just signposting to the website. I didn’t need to mention ‘digital inclusion’ to her, even though it’s just one of the many priorities in the NHS. She knows her patients and how many of them still walk in for help and quickly offered an alternative support option. That is inviting them in, yes?

Next up, in a change of order, I decided on Elizabeth Buie’s talk ‘Older Adults: Are we really designing for our future selves?’
I’m (just) entering the category of ‘older people’, although as Elizabeth described, even agreement of who is old, offers variation in studies. I like to think I’m on the younger end of old. Wonderful, personal insights brought this session to life, with a bit of audience participation on who could hear (or not) the audio files linking age to changes in hearing capability. The best bit for me was understanding the difference between ‘fluid and crystallised intelligence’ as our ability to remember, learn and process may slow down, yet our knowledge from experience and education remains throughout life. I hear the term ‘subject matter expert’ often in the NHS and I’m sometimes asked in our team, to coach and pass on knowledge to our newer, younger colleagues. I also get to guide NHS commissioners on how to ‘deliver their priorities’ with general practice. But sharing 40 years of work in change, quality and improvement then knowing which bits are relevant, when to offer and who to, can’t quite be distilled onto an A4 product sheet, or a simple checklist. It’s much more nuanced. I know that the stuff I have experienced comes at random from my memory bank, whist I can forget in 5 mins what I’ve just been present in. Thank you, Elizabeth, for taking me back to the clicking keys of the typewriter and explaining why the ‘qwerty’ keyboard originated because the keys stuck on the most frequently used letters. Even though I know the order of an alphabet, car parking payment machines ordered by alphabet not qwerty, can raise my blood pressure!

Linking this to the workplace where we have the possibility to use voice to text software, yet we are still advocating training in touch typing for clinicians, seems like a missed opportunity. Thinking about dexterity, knowledge, and experience, then watching GPs who may have trained 30 years ago to quickly scan-read discharge letters for key pieces of information, seeing them struggle to navigate this same information in a variety of formats on multiple screens, seems a punishment we should address as a priority. Especially, if we are to improve the user experience of corresponding between healthcare providers. Watching people then retype (with errors) a summary of that information into another clinical system, slowly with two or three fingers is heart breaking, when many have used voice/dictation systems for years for their own letters, and the sending consultant in the hospital probably did the same. Even considering when a consultation is being spoken between patient and practitioner, then typed up rather than recorded as audio, or converted to data and narrative to meet the needs of data transfer, task allocation and patient information. There is a research project here for sure.
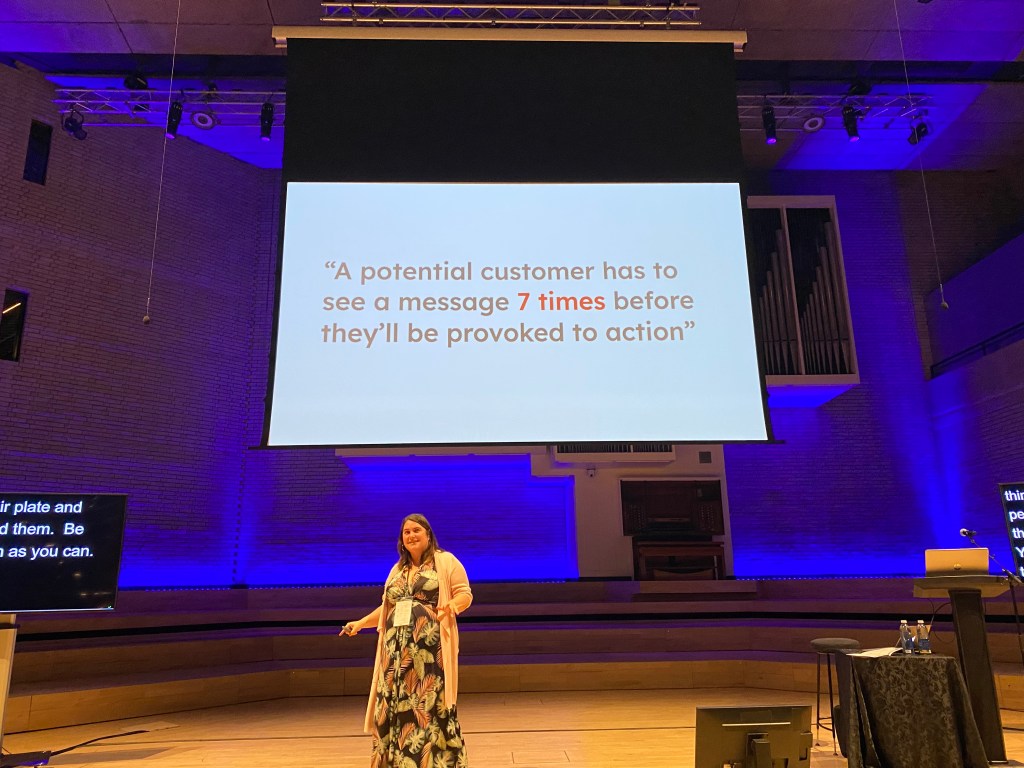
The afternoon sessions did not disappoint either. Audree Fletcher’s ‘Designing in the dark’ gave me many notes to take home, but this one message was a big one. A potential customer has to see a message 7 times before they’ll be provoked to action.
Audree reminded us that winning the big goals takes time, and finding the ways to achieve this is a lot more complex than just pitching your idea and hoping for the best. As someone who can get disheartened when others don’t just come with me, the hints and tips and final canvas gave practical suggestions to help. Understanding what else is going on in other peoples’ worlds, knowing the competition for funds, connecting the proposition to ‘what matters to them’, finding the right channels to drip feed the message, are all great ideas to get pitch over the line. I have loads of ideas how to make things better, then get dejected when they disappear into a dark NHS hole and layers of ‘commissioning by committee’. Meanwhile we lose months of progress whilst people ponder the relative value of this proposal over another. The NHS is amid yet another reorganisation, and many decision makers are involved in their own personal worlds of survival right now. Yes, I need to put myself in their shoes, but maybe it’s ok to also bring them out into the shoes of the people that they are supposed to be commissioning services for.

Example of using ChatGPT to explore bias associated in existing data, see the affects of pronouns he/she to same question, about who is working hard enough. @mmitchell_ai
Sarah Knowles and Lynn Laidlaw’s discussions of Data Feminism and challenging power along with where the patient sits in all this change, got a big thumbs up. As a sociologist, this talk touched my heart. Hearing Lynn question the ‘burden’ of healthcare and why it is considered as ‘work’ for practitioners but somehow described differently for patients, reminded me to challenge people with power, to acknowledge their privilege and share it out a bit more. Who has the power in the room should always be on our minds and it was great to see some familiar quotes and the effects of binaries, hierarchy and bias in our work.
The final keynote did not disappoint as data visualisation specialist Nadiah Bremer took us through constellations of data to rethink how we see connections. In amongst other more significant stuff, Nadiah represented the connections of google searches about cats and dogs in a beautiful way.
I’m watching some parts of the NHS gets it knickers in big knots over data right now, with an unhealthy focus on counting the wrong things and making erroneous connections. One attendee astutely observed that this final session, joined the dots across everything throughout the day together; research, experience, emotion, inclusion, context, power and data. Powerful stuff.
And so back to my earlier part of the week, I’ve managed to resolve some of the problems, but it still feels like I’m wading through treacle. I now better understand my new cloud hosted, telephone system call flow design, following a further phone call to the supplier. More edits are required to simplify for the user but still provide me with a whole load of data to understand.
My ‘Test patient’ for the NHS App, is no longer a Dummy patient, it’s a live Test patient in EMIS, even though I still can’t associate it with NHS App.
My Friends and Family data is now successfully uploaded into the bean counting system so we no longer have a big red mark against the practice, even though it’s an extremely crude mechanism to measure patient’s experience and I now have the 2023 General Practice patient survey to review.
For the people I work with in the NHS, you see this data stuff – we have a bit of a plan for you….watch this space.

And finally, although she may not realise it, I also get to take my sister to work.
