As the year starts to wind down for the holiday period and more people share their year’s highlights, I have a slightly different post this time. Its less about work and more about the personal.
In my old job as a Practice Manager, I enjoyed writing my annual newsletter to the team, to thank everyone for their hard work, to reflect on the milestones and achievements of the year, to acknowledge the special people who had joined or left our team, and also to include what was coming up in the next year. I’ve never done that at Redmoor, maybe because I as always felt I was in the team, rather than the Team Leader.
This year has been full of ‘stuff’ – events, milestones, launches, people joining, others moving on, NHS reorganisations (again), new Government etc. But I’ve come to the realisation, that whilst these lovely people will always be amazing friends, some of the work stuff is less important to me these days, and that I have other things to think about, take joy from and look forward to.
A few family and life events have really sharpened my focus on what I want to spend more time doing. When I look in a mirror and an older larger version looks back at me, I’m not sure I recognise myself, because in my head, I’m less wrinkly, and obviously a different shape. The mirror is reminding me that my life clock is ticking on though.
We are moving home in the New Year, and clearing out the loft, garage, kids rooms (they are now grown men), finding photos, favourite toys, school homework and special books has resulted in lots of wonderful memories surfacing, along with a few tears. Anyone who has moved house will recognise this; it’s not wrong to say that its one of the most stressful times of your life. Currently dealing with 4 solicitors, 2 estate agents, planners, then removal companies, arranging and travelling the ferry is brain draining. Trying to do it all in the evening and weekends, after a full week’s work is just hard work – solicitors must wonder ‘who is this mad woman that emails at 5am’. And I’m a bit tired.
So, after discussing my life priorities with Marc and Matt, we’ve agreed that I refocus on just a few key things, that allow me more flexibility and still provide Redmoor with the help that I can do easily. I am grateful for their understanding so, I’ll be scaling back any operational and public-facing work and watching others take centre stage, with proud encouragement from the wings.
Practical as ever, when I move, I’ll have rubbish broadband and in the current climate, I don’t feel like lining Musk’s pockets for Starlink just yet.
Also, when you work in health, it’s too easy to forget your own health and I’ve got to get fitter and stronger quickly for our family trip to the slopes in February, as I don’t want to be holding people back. I will have the joy of seeing my two fabulous nieces catch up with my sons again, and watching my youngest in his element in the powder, forging his own future, as Jasper rebuilds itself after the forest fires last year.
As the spring approaches, I have my bulbs in pots and plants ready for the new garden, and I’m already planning the best place for a few more chickens – I’d flipping love a goat or two but that might stretch Mr D’s tolerance. He’s got his sights set on the new golf course and I have many beaches and forests to walk with my eldest son and his brood of dogs.
So, I’m swapping my evening sunset views with a glass of wine, for these new morning sunrises and maybe the yoga mat, and that feels like a good omen – getting up each day to enjoy more nature and much as I love the team, hearing less Teams calls.
Now these 3 are ready for their breakfast, so I’d better get cracking for the day. It’s our Christmas Quiz tonight, so its Christmas Jumper day
I’m sure most of you will have seen the promotion, if not – here’s the Digital Primary Care Fest webpage again to see what you might have missed. Most of the content is being shared on the new Digital and Transformation network, so please join over 200 new users in the last two weeks, and chat along with like minded people who have questions and ideas to help each other.
Anyone who has organised a week of events will know the required planning and how much effort this takes. Not the wisest thing to do, but popping in 10 day holiday away and landing back in the UK a week before meant it was full steam ahead on my return. Although this added a certain amount of frisson, I’d recommend you avoid doing the same. Our team of keen and dedicated people, put in the effort to make the week a success, and judging by some of the comments on socials, I think everyone found something of use. And that’s what it’s all about, meeting people in similar roles, I think I saw the phrase ‘like-minded’ a lot, and the general energy throughout the days demonstrated that people had things to share and wanted to learn from each other.
GP Provider Collaboratives (often built from Federations and Alliances of practices) in some areas still seem to be missing out of the ‘engagement’ loop in between ICBs and Practices/PCNs. In addition to being Providers in their own right, for Enhanced Access and other ‘at scale’ services, many also employ the Additional Roles and the workforce element is resource heavy for them. As ‘membership’ or representative organisations, they have a crucial role in engaging with their practices, which Commissioners could and should exploit. This seems particularly important when trying to deliver consistency of services and access, across neighbourhood teams or using common digital products within networks, to offer equity of access beyond core hours.
The ability to communicate at scale is also an opportunity. Federations and Collaboratives can do this and ensure consistent information is delivered about primary care services at ‘Place’ or neighbourhoods, supporting practices and PCNs, using content shared across Websites and Social Media. Listening to the conversation about GP websites, I was transported back to 2017 and watching 9 practices independently create their own version of information about a new same day service, then posting it separately on 9 different websites. I’m not suggesting a separate website is needed for Enhanced Access, but I am still suggesting that content is created by the service provider, then pushed out once, across a common website platform, directed to and from GP websites, which is where patients will look to find out about appointment availability. It’s still uncommon to see fully integrated evening and weekend appointment availability with the full primary care team, accessible to book online via a GP website. Whilst there are great examples around where some Feds have got a hold of this, most are still on the first page.
Data – who’s uses it and why?
On both the GP Collaborative day and the DTL day, I shared our Digital Maturity Index, which we have just refreshed to include Online consultations and will incorporate telephony data in the new year. There was acknowledgement in the room about the variation across practices, with nods of recognition of practices who may be further behind on their digital journey. We always have an interesting discussion when I compare GP survey responses against Digital access. But looking at the Registration with a GP Surgery and spotting where Collaboratives can support working beyond just the practice, we could see opportunities to help with coding and summarising, also smoothing the Registration process across the practices. Someone suggested that the ICB would find this data useful, and yes, perhaps through the lens of contract monitoring, I’m sure they would. At the same time, the Collaboratives and PCNs will be impacted by the success or failure of their member practices. Relationships still seem to be a source of tension, as different primary care provider organisations work out their purpose and collective benefits.
The DTL (Digital & Transformation Lead) day.
We wanted this to be a day where DTLs shared their challenges, helped each other, offering suggestions about things that had worked well, and the DTLs were certainly active in this process. I don’t know why, but I was surprised how many DTLs were ex or still acting Practice Managers. I would have looked to move into that role myself if I’d not already joined Redmoor and we lost two great colleagues to the role when the jobs were first created. The DTL role is very much like practice management, hearing comments about feeling ‘quite isolated’, and needing to influence stakeholders at varying levels of seniority across organisations (ICBs, Clinical Directors, GP Partners, PCN managers, & practice teams). Not so easy to do though, when not necessarily directly managing. Others expressed a lack of clarity of expectation of the role both from commissioning and provider organisations, without much structure for development and very much relying on own resilience. Some great ideas came through to maximise income for practices and PCNs, while still ‘ticking the ICB contract boxes’, and delivering time-saving initiatives in practice, that improve the patient experience. I’m sure my colleague Dillon Sykes will have a blog coming out about his last two weeks, so I’ll leave him to share his thoughts too.
Now for the #Hackathon
The GPT Hackathon day was just the best for me, largely helped by the people in the room who needed little prompting to show their innovations. It was great to catch up with and see many familiar faces and to meet new people, whom I’ve only known online. As ever, the quality of the speakers and contributors kickstarted the thinking, with the morning devoted to learning all about AI and GPTs and the afternoon spent putting that learning into practice to come up with use cases. A big thank you to Dr Keith Grimes, Curistica, and Chris Bush and Lee Valentine, Nexer Digital. We had a range of Tech enthusiasts, patient representatives, and inclusion specialists with us, alongside people who wanted to explore how GPTs could support them in daytime workload. Some great ideas were sent in beforehand, in case the teams in the room ran dry of ideas, but a few wanted to use the opportunity to pitch ideas, before breaking out into groups to build. I was amazed at how quickly everyone put the morning’s learning to good use and all teams delivered a solution in just 1.5 hrs.
My colleagues Matt, Clare, Dillon, Stacey and Leoni were able assistants on the day and Matt recorded most of the sessions. You can find Matt’s more detailed blog from the day containing the slides and videos if you want to have a more detailed look.
The learning for me is that we have a void of ‘governance’ that is leading to caution in many and on the flip side, people possibly working outside the ‘safety zone’, not understanding the risks or personal liabilities. One of the hacks was to create an AI marketplace, where people could visit to find out more, where suppliers could offer support and clinical safety, alongside governance guidance. They built a quick GPT for suppliers to check if their product needed DCB0129 & DCB0160. I can see a need for a follow-up round table event with representatives from ICO, CQC, Regulators, Medical Defence unions, Medical, Nursing & Management representative organisations, alongside NHS as Commissioners and Standards organisations. Then we can explore where the concerns may be, what the actual risks and liabilities are vs those as perceived and who these currently sit with, and who they might be covered by in the future. Until we move this away from independent practitioners to the wider NHS system, we cant harness the opportunities that AI can bring or manage the safety at scale. I posted on the NHS AI forum afterward and the suggestion of building an ‘AI Charter’ together might help us all.
As we approach the end of the first quarter of a new Government, I’m taking a moment to reflect on a few papers and articles released and considering these against my experience of trying to use and implement Digital in the NHS.
I’m sure many of you will have seen or commented on the recent paper ‘Preparing the NHS for the AI Era: A Digital Health Record for Every Citizen’, as part of the Future of Britain policy initiatives. As usual, it was met with the full range of commentary, from enthusiasm and welcome support to the obligatory dumbing down headline about ‘chatbots doctors’. Dr Charlotte Refsum, Director of Health Policy, Tony Blair Institute for Global Change summarises the key points in her LinkedIn post (which is where most of my blog readers get their information these days since the demise of X – but that’s another story!)
Please can we fix the basic requirements first?
I totally understand the response: ‘Please can we fix the basic requirements first’. One of the biggest surprises when I joined the NHS 20+ years ago, was that the basic user requirements for tech were at least 5-10 years behind the nuclear industry that I had worked in previously. I recall being astounded at having to submit a business case for a £250 desktop multi-function printer/scanner to save hours standing at a photocopier, printing patient records, then re-typing that information into templates to be sent by email, and then yes, posting the paper records to the PCT HQ. My request didn’t get approved – I moved on.
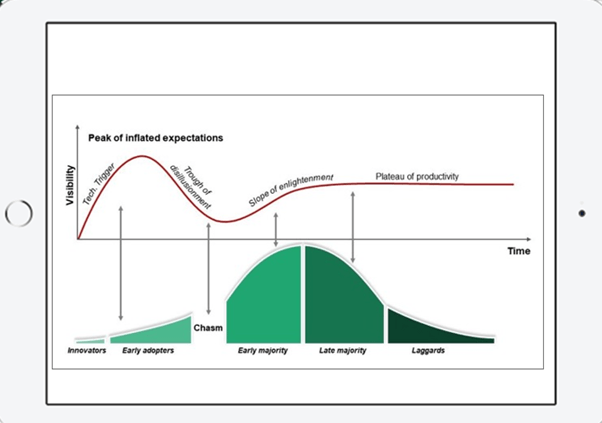
During those 20 years, we have seen variable improvements, some big-scale projects start, get delayed and then scrapped, and a lot of money paid for products not used. I use this image regularly in my presentations and it feels like the gap between the early adopters and laggards seems to be widening, as well as the hype increasing, quickly followed by the trough of disillusionment. I still take part in video meetings with practice teams, all huddled around one PC. No spider phone, or owl camera in the meeting rooms, and some don’t even have a webcam and headset to participate fully.
The Citizens Digital Health Record (DHR) and Primary/Secondary Care interface
I’ve been an advocate of patients having access to their full medical records for 10+ years since I worked in practice and could see the value to patients as well as to our workload. However, creating a new multi-sector DHR in light of the legitimate concerns around procurement and data security is not without challenges. Seeing the attempts to share and view patient data across health systems has been soul-destroying in some instances. The requirements of PCARP – ‘cutting bureaucracy’ and addressing the challenges of the primary/secondary care interface seem to be thorny too, with the bureaucratic referral process incorporated in the BMA collective action guidance. As a Commissioner in Cumbria in 2008 looking at part of this work, I recall a discussion with an Orthopaedic consultant defining the pre-surgery baseline test information they required. I asked why Primary Care couldn’t just create and supply a ‘view’ from the relevant part of the GP clinical system to Secondary Care. It has been technically possible for some time, but still not done. I still see each ICB or Region reinventing this wheel or worse, not addressing this issue at all.
The Technology Innovation Framework ‘new market entrant’ clinical system suppliers are still building functionality to send and receive ‘documents’ into and out of hospitals because they have to design the new systems to ‘fit’ with existing NHS systems and workflow. Secretaries spend hours listening to digital audio recordings and populating templates, administrators uploading or archiving the same, all to ensure the correct coded data is sent from A to B, or to make sure payments can be attributed for the work. This is light years behind where it needs to be in thinking and design. Why are they not designing these new systems to allow secure structured data flow and visibility, separated from ‘task handovers’, with a ‘patient friendly’ version alongside? I’m sure many of us have looked at our records in the NHS App and wondered what on earth some bits of it mean. So now, I’d say that people need access to their ‘health information’, not their ‘medical records’ – its subtly different. Clinicians need medical information in order to advise or treat, Managers need a different set again. Transferring care, is different from the information that patients need, as is the need to track flow of activity for demand, capacity and resourcing, and then capturing outcome data to check that the intervention works. It surely cant all sit in one DHR, can it?
Lord Darzi’s review
There will be many that comment on yesterday’s release of the Independent investigation of the National Health Service in England, AKA the Darzi review, for many it contains no surprises. This review along with numerous papers and articles all feature Tech or ‘Digital, not Analogue’, and AI as a central part of the solution. Those of us involved with change, implementation, and optimisation know, that the Tech alone will not suffice. Having the headspace to think differently, when you’re up against the clock, or burning out so you can’t even consider taking the risk of doing something new, all needs to be factored in alongside the Tech. Let alone addressing the working across silos.
Exhilarating and terrifying – not just the internet, but AI
Then I came across this old clip of David Bowie predicting the impact of the internet in 1999 and I have to say, I can have similar feelings about AI – it’s both ‘exhilarating and terrifying’ at the same time. I can get enthusiastic when I have a call like the one I’ve just had about predictive analytics, taking millions of data points and using AI to understand the trends. At the other end of this, I do more than roll my eyes when I see glib predictions that AI will solve all our problems, or replace the need for people, or be the only source of the truth.
Having worked with patient and staff data, and understanding the requirements of data controllership, the risk of data breaches seems a priority, closely aligned with clinical safety and acknowledging bias in all its forms. All the marketing hype is about efficiency, so it is great to see sensible guidance being released.
As the system strives to move more and more services to digital platforms, leaving people behind, who may already be digitally excluded and suffer poorer health outcomes as a consequence, is equally important. Nexer Digital offers practical service design advice in this blog post by Chris Bush; AI for all; Inclusive design principles for the use on AI in the Public Sector and Danny Lancaster offers us real-world use cases to help us consider how AI tools can support a more inclusive workplace, not just a more efficient one.
So, with all of this in mind, we’ve decided to get the experts in the room and see how we can solve some of the core General Practice problems, using AI safely, inclusively, and effectively. When we asked people to tell us what problems they like addressed, it’s the mundane, repetitive, time-consuming things, not the boundary-pushing stuff.
If you’d like to join us at our Custom GPT Hackathon on 3rd Oct in Leeds, to learn, share knowledge, and maybe enjoy a pizza even whilst having fun, why not come along and find out which side of the David Bowie ‘AI line in the sand’ you’re on?
Meanwhile, I’m leaving you with an image of Dr Keith Grimes, staying up all night testing the new ChatGPT models in preparation.
Getting the best out of remote and digital general practice
Some of you will know I live in beautiful scenic Cumbria. So, you’ll have an understanding all about lack of public transport and how flipping hard it is to get anywhere in a hurry.
Some of you will also know that I have a touch of FOMO, so when I get an invite to two things at the same time, I struggle to decide and often think, maybe I can do both.
The dilemma
Our Redmoor team were having a redesign session on 24th April, partly in response to some NHS contract changes, partly because we’re 12month into one programme and 3years into another and we wanted to reflect. Also, because we want to look forward and make sure that our products and services support a hugely stressed system in General Practice, and we have the expertise in the team to help.
Then, I get this invite to an event presenting the findings of quality research by the teams at Oxford, Plymouth and the Nuffield Trust, delivered in the House of Commons, for MPs to listen in order to understand the issues and complexity of modern general practice remote care. The research team have created this summary to share, so that others can learn from the 2-year study and build the findings into their work.
I’ve been involved on the edges, as part of the expert advisory group and as a participant in a series of workshops, but this is very much part of my everyday work and something I’ve been passionate about in the NHS for many years. How could I turn that invite down.
I decided to attempt to do both sessions. One from the train, the other in person.
Plan for the unexpected
What I didn’t plan for was a horse event, total disruption to the road network, and it being ‘surgery day’ at the House of Commons, resulting in the longest queue to get in, the fastest transit through the building and security, and arriving just slightly late for the session (along with three others, reassuringly – I wasn’t the only person who mis-planned). For those expecting selfies with the Ministers – no time for that I’m afraid.
The event in person
During the presentation, hearing the personal stories of those affected by ‘Remote by Default’, as receivers and providers of services, will always bring you down to earth, irrespective of the magnitude of the setting.
Professor Trish Greenhalgh and Dr Emma Ladds sharing some of the experiences from the research
The strongest message I heard is that people need and value continuity of care to get the most from the experience, prioritised over quick ‘transactional’ access. Secondly, that delivering and receiving care remotely (telephone, online, video, asynchronously) can be safe (see Table, p10) but that training and developing the right culture is as fragmented as the technology used to deliver care. Thirdly, that the purchasing of technology is not just about the product, but the variability of its implementation has resulted in unequal impact (see my other blogposts). Finally, that although the NHS has plans to embed this into education, it will take a long time, and General Practice need the help now.
So, the training needs and competency framework are super helpful, and for those supporting general practice this research is gold dust, as it should inform the basis of any training and advice.
We’ve already used this patient facing communication created by the researchers and posted out a social media campaign across 700+ practices to over 30k patients to inform and encourage people to access care this way.
How to get the most from
Although it was a flying visit, I met and hugged some incredible people that I’ve only ever seen on screen or interacted over socials. I sat beside someone who also hailed from the North and it transpired that I knew their father – how Cumbrian is that!
What happens next
The research team are sharing their learning on a public zoom event on 22nd May, so watch out for details if you’d like to join us.
The event from the train
Back at the Redmoor office, the team had a successful day too and now have a clear plan for our digital and transformation products and services, so watch out over the coming weeks/months for updates.
We took part in our joint HSJ Awards - Best Consultancy Partnerships interview with one of our clients this week, as we come towards the end of a 3-year programme. As one of the original gang at Redmoor Health, it was nice for me to reflect on the successes of a strong relationship, developed to deliver a long, multi project programme aimed at increasing digital access, improving patient communications, upskilling the workforce and supporting the Digital First team to deliver their aims. I took a moment to consider this strategic partnership against the current climate of change and chaos in Primary care and thought I’d share some musings with you. BTW, its 8mins long so get yourself a brew and ponder with me.
Finances
Its that’s time of year, when in the last quarter, there is traditionally a frenzy of activity in General Practice. Teams are chasing patients and are working hard to recoup any finances earned throughout the year to maximize payments, following delivery through QOF and the Primary Care Network contract. With only 7 weeks to go to the new financial year, uncertainty over pay and contract negotiations is making next year’s planning harder than usual.
Throughout 2023, there was a raft of new guidance, contract and service changes that managers needed to understand. ICBs and Regions are now comparing progress against targets and seeking assurance or evidence of improvements against new criteria before they can release payments. Some are excelling at this, others finding it hard work. That’s on top of the usual round of ‘heck, we have to spend this money before year end’ last minute decisions. Previously, we’d agree with our clients to receive and hold this year’s £s, then together work up a more detailed scope for delivery into the new financial year, when their priorities are a bit clearer and they can engage properly when primary care have more time. With the reorganisation and requirement for a 30% reduction in costs across NHS Regions and ICBs, some people are facing redundancy or moves to other jobs, consequentially, loss of local organisational knowledge and decision-making inertia is becoming clear. Also, the combining of primary care transformation and digital budgets is affecting financial flows and prioritisation of projects. Clawbacks on unspent budgets are being mentioned in dark corridors and on socials, which is a sad reflection both on the plans and especially when primary care need the funding right now.
Primary care contracts
One element of the PCN contract is the capacity access and improvement payment. Unsurprisingly (clue is in the name) this is largely about improving patients experience and access, with payments linked to improved appointment recording. As part of our Digital Managed Service, our team have been supporting PCNs to deliver this guidance, contract changes and ‘new models of care’, so my super colleague Dillon Sykes and I thought this might be a topic for discussion at our session at Best Practice, London on 28 & 29th February. We’ll explore some of the headlines, overlaps and gaps, ponder a little around the various checklists and criteria to be met, then hopefully share some practical steps to help.
We are seeing lots of angst that the General Practice Appointment Data (GPAD) dashboard still seems to contain inaccuracies and a lack of clarity over what is counted, and how to make historic changes etc that will impact on payments. New to the ‘additional roles’ stables are the Digital &Transformation Leads and alongside PCN Managers, both are still trying to understand appointment mapping guidance released in 2021. Clinical system providers have released workarounds in the last couple of months as temporary fixes. Frustrations are appearing between General Practice and PCNs as the data is held and configured at practice level, but the impact is felt in the PCN.
It’s great to hear that some ICBs are supporting well, providing datasets throughout the year to keep an eye on progress. We are sincerely hoping that ICBs take a pragmatic approach to releasing the final 30% payment, whilst the data is still ‘more than a bit flaky’ (technical term).
To help with GPAD, our team ran webinars and held 1-1 sessions with practices or new D&T Leads to go through their configuration and data. We produced a simple GPAD tool to help navigate the guidance and we’ve also asked passed on quite a few questions to people in NHSD/E to gain clarity.
Procurement of new digital solutions
This last year’s quarter is also a little bit different though, for many suppliers of services and products to the NHS. It’s not unusual for slippage in the NHS, but some of the key elements of the Delivery plan for recovering access to primary care that slipped or were reprioritised, will have knock-on consequences for many colleagues in the product and supplier landscape. This will also affect practice teams and inevitably, on patient services.
I’m fortunate to occasionally take part in user research and know the NHS team are working hard to make the experience of the buying catalogue better, but this delay has impacted on ICBs, PCNs, Practices, Product suppliers and support organisations like Redmoor. Part of my job is to seek out new partnerships and products that will help to improve General Practice, and I love chatting with new suppliers to find out how their solution will help. There are a few with products that will knock your socks off but are not available to purchase from the existing procurement frameworks. Some PCNs are bravely buying directly, as they can already see the value, but many are nervous or don’t have the finances to buy direct, especially if their local ICB is expected to and will fund (or even part fund), once the new buying catalogue is available.
As a consequence of the delay, it looks like many commissioners have little choice but to extend existing digital solution contracts for another year. This can leave practices with products that they didn’t choose or don’t use and patients don’t like to use, so stick with the conventional methods of access (Telephone). So, in ‘kicking the can down the road’, existing suppliers breathe a sigh of relief and new products don’t get into the market, leaving us all feeling just a little bit frustrated at what might have been for another year. Do we invest time and energy trying to optimise solutions that we know don’t fit the needs of our staff and patients?
Our new procurement support service logo
Suppliers tell me they have lots of interest from ICBs and PCNs but can’t recruit to scale up delivery until they know the contracts have landed. There will be a rush at the end, and we know deployment and implementation will suffer. These tools are essential to deliver high quality 21st century primary care. Having been through this process with one of our strategic clients last year, we have experience and are well positioned to support suppliers and ICBs with market and practice engagement, early implementation, adoption and spread. So, if you want to plan early, drop us a line and we’ll walk you through how we can help.
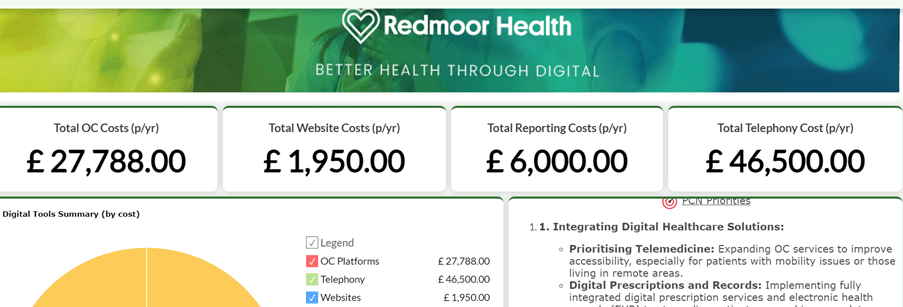
An example PCN dashboard showing the costs and variation of products in use.
Research
In addition to user research for products, I also contribute to research for new services in development and I’m delighted that NHS are developing a guide to improving messaging. This has become such a complex area, since the inclusion of messaging as a requirement for all online consulting tools. The NHS is paying twice for quite a few functionalities and the holy grail for practices was always to have digital solutions in just one platform. There are a couple of suppliers doing this extremely well, and with the increasing desire to reduce SMS costs, data messaging is the way forward for many. One super research project that I’ve had a small involvement as part of their Expert Advisory Group is the Remote by Default project from the teams at University of Oxford and Nuffield Department of Primary Care Health Sciences. They’ve released some great resources following a 2 year study into remote care. We’ll be helping to push these out to patients in over 700 practices via our Social Media managed service, and will build the training competencies into our programmes, so we are confident that our work is grounded in rich research. What is interesting, is the different approaches across the Nations. Scotland have procured one video consulting platform for the whole nation to use, with a contract to 2026. This means they have one set of patient facing resources and one training platform for all practices and users. Very different to our market place approach in England and probably a lot less confusing.
Now – lets’ talk telephones
As another example of what I’ve just described in the procurement section, lets have a look at the requirement for Advanced Cloud Based Telephony. Seen by some as the panacea to ‘the 8am rush’ and made a requirement in the GP Contract by end of 2025. The Better Purchasing Framework was issued, some ICBs took advice and started to plan the ‘at scale approach’, working out whole system requirements, engaging with practices and PCNs to gain advantages of greater purchasing power, optimise local infrastructure and achieve some consistency of service offer – great stuff! Then a letter appeared late Nov, expecting all practices to sign up by 15th Dec 2023 or they would miss out on the funding opportunity. Thankfully, someone realised the well-earned Christmas and New Year holiday was looming and the deadline to select a supplier was moved to 15 January 2024, with a signed contract by 2 February 2024 and go-live by 25 March 2024, with all features in place by April 2024 at the latest. Just another added pressure in the last quarter of the year.
Now there is anxiety over where the costs will land, and we had a flurry of requests to help people make a choice urgently, so they didn’t lose out on funding. We had others that had already moved to cloud telephony before the contract requirement was released, but had chosen suppliers not on the framework, so maybe didn’t have all the features mandated in the new contract. Some practices had been earlier adopters, made the investment then found that there was support to buy out of existing analogue contracts. Or course, anyone that has ever implemented new technology knows you can’t do it in a rush without good planning. Then after deployment comes the real fun – how to make it work for you. We saw this happen during the pandemic with the necessary but rushed roll out of online consultations.
Our team have been delivering workshops, listening to and improving auto attendant messages, optimising call flows, aligning with online service options, all to ensure fair access to services and an improved experience for patients. And then of course we threw in a Digital Journey Planner module around planning and optimising Telephony.
Example Call Flow options with routing out to alternative and online services
This is just a flavour of our support on offer to help the NHS at all levels in primary care to navigate the noise, help with the priorities, support the providers to deliver, optimising the solutions available. We hope you can come and see us at Best Practice at the end of the month, we’ll be at Stand D45 talking all things primary care improvement.
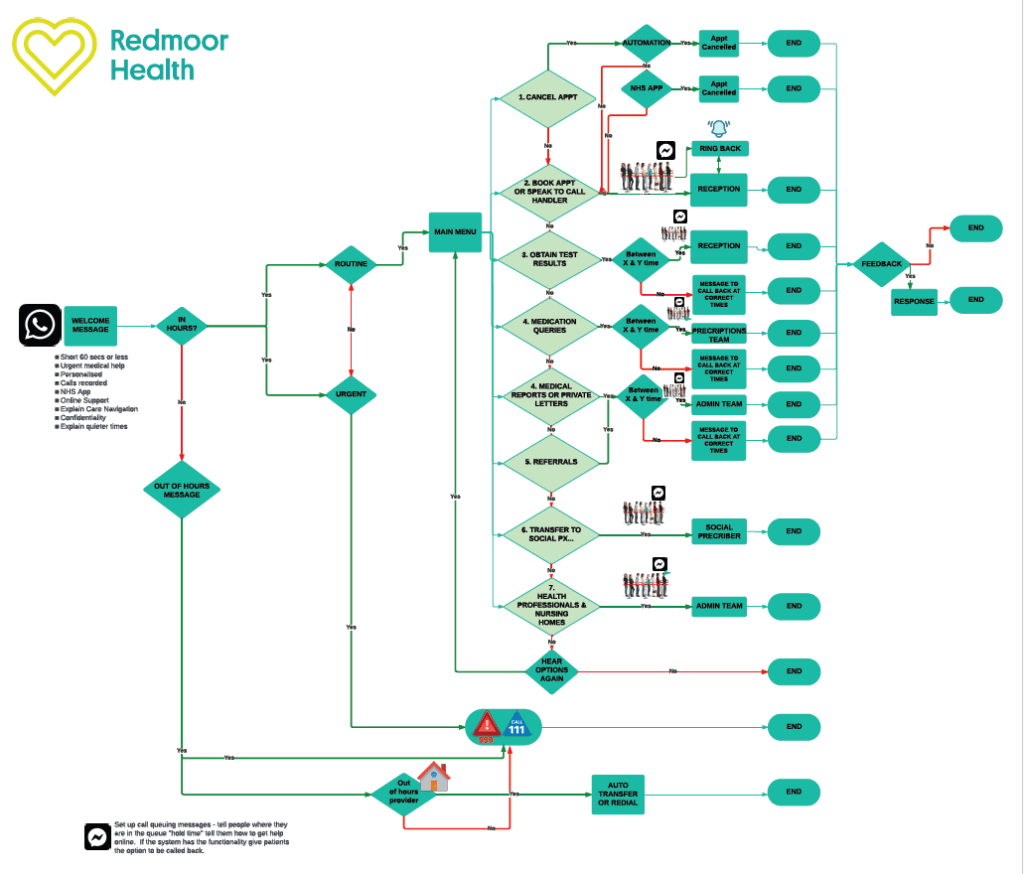
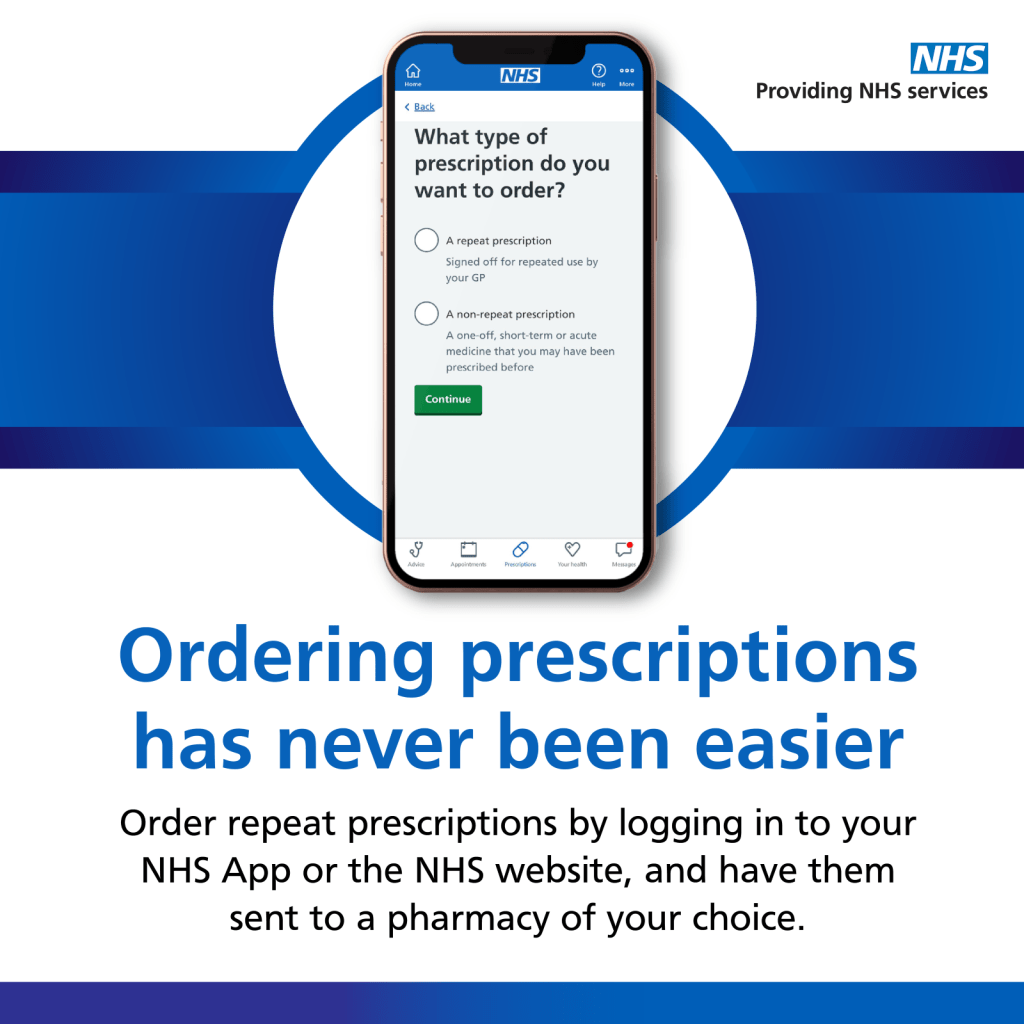
At Redmoor Health, we’ve been helping practice teams, the wider NHS and communities to support patients to ‘get online’ to access health services for several years now. We have also been out and about this year at various events asking the question, ‘Does your digital front door revolve?’.
Slide from Presentation at Best Practice Event, Birmingham – ‘Does your digital front door revolve?’
We ask this question in relation to the experience of patients who report their online user journey as ‘going around in circles’. Similarly, as providers in healthcare, the NHS has access to a myriad of digital products, not always well designed or interconnected, that occasionally send people shooting off in directions they weren’t expecting or losing them on the way to finding help. Primary care staff often ask us for help to understand all the features across different software and systems and how to get the best out of them together.
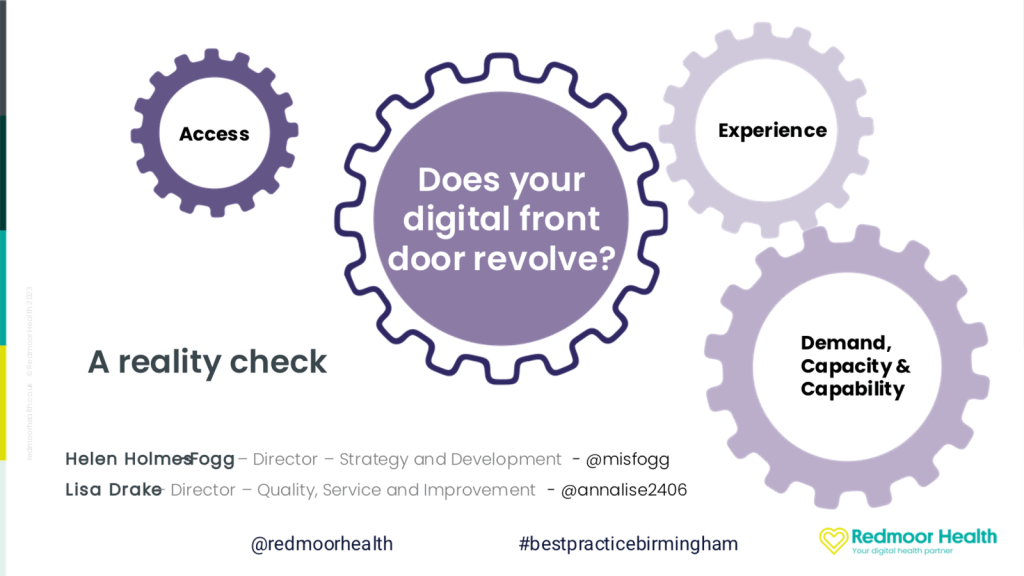
So, I’m delighted to see the announcement that the NHS App is being redesigned, following extensive user research to improve that journey and to become the essential part of the digital front door, along with good websites, making entry into NHS care easier.
Slide showing images of Welcome screen and Messages screen for new NHS App design, with labels to show users what the changes will look like
From 12th Dec, NHS App users will be prompted to update their App and will start to see some changes, making things simpler to navigate, with clearer language and a more intuitive experience – wonderful stuff!
The NHS set a target of 75% of the adult population in England to be registered to use the NHS App and NHS website by March 2024. That’s a big ambition, especially with over 10m of the population still lacking the most basic digital skills, according to Good Things Foundation Digital Nation UK 2023. It’s also not so easy to ask patients to move from another App that they have used successfully for several years, to something new when they can’t see any additional benefit.
We thought we would offer you some help along the way to achieve this target. You might consider this a late Black Friday, a Cyber Monday or even an early January Sale deal from the team at Redmoor Health.
In Jan, we will host a couple of free webinars not only to walk you through the changes, describing the additional benefits, not just for patients but for practice staff too, in terms of time saved and an easier workflow.
For anyone still wondering what to do for their QOF (quality outcomes framework) quality improvement project in practice or PCN (primary care network), we have a simple action plan to help you to increase the numbers of patients who order their medication online.
The quality improvement plan to increase NHS App usage, linked to Digital journey planner, with smart goals for improvement
We can help you to to find your data as a baseline, so you can show the improvement and help to secure your 30% funding against the capacity access and improvement plans.
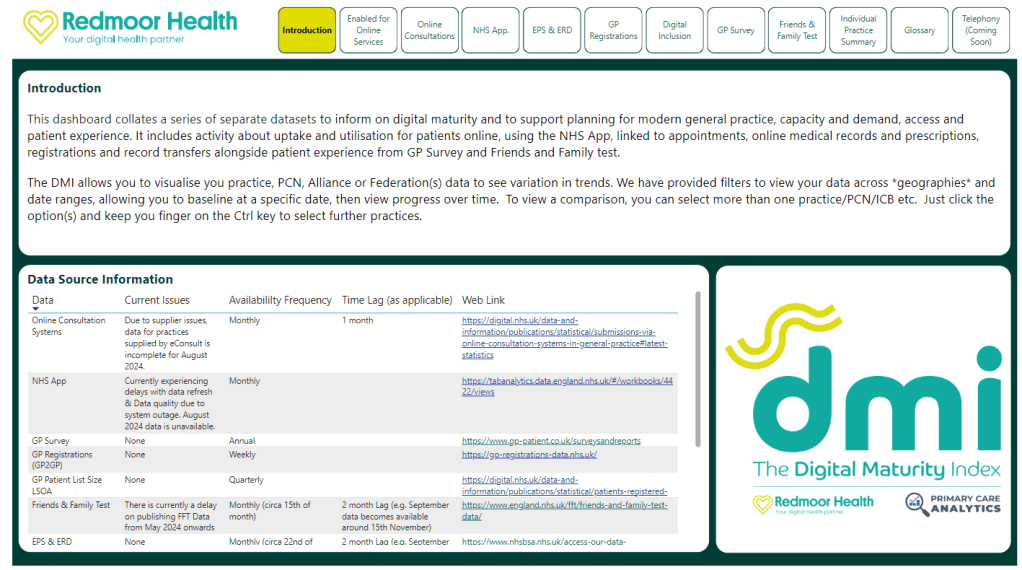
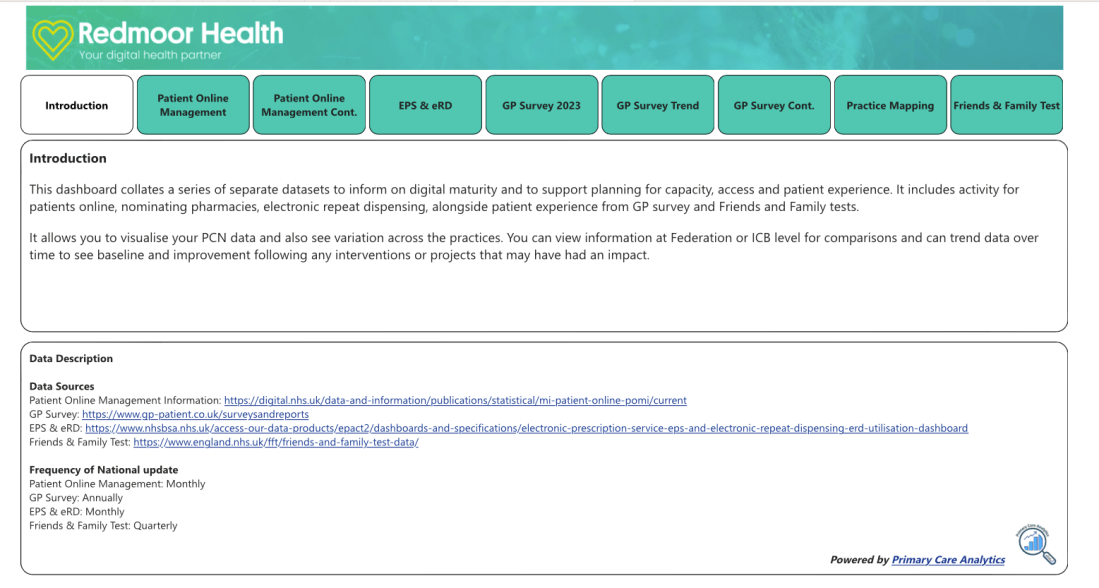
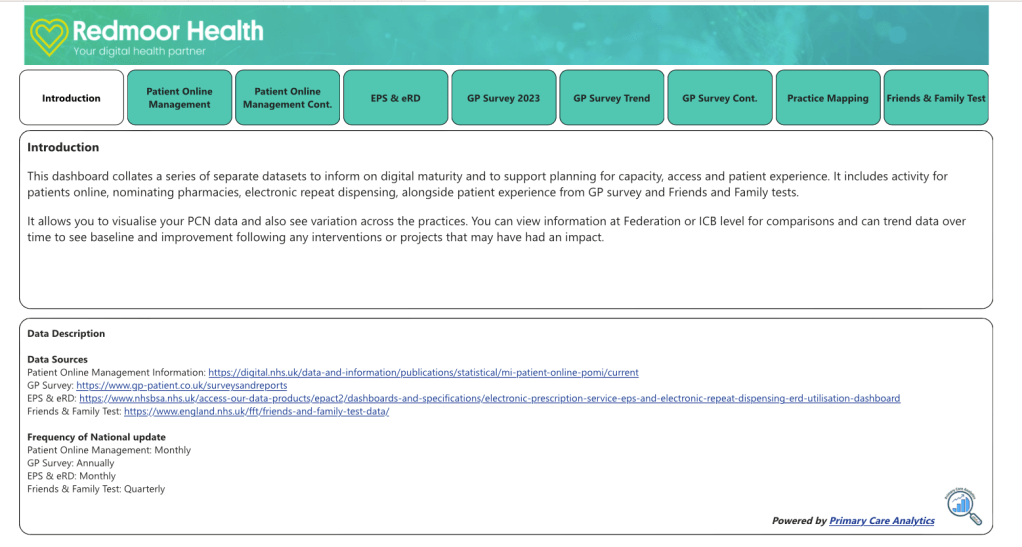
Polite plea to the NHS App data people – how about providing the data out in the open, instead of behind this dashboard and let us help you to share it widely through our digital maturity index. If you are curious, have a quick look at this explanatory DMI video, where we have just added NHS App as a separate dataset, helping practices to see all of their available ‘online data’ in one place.
Digital maturity index dashboard, containing various online datasets, including NHS App
In addition to the content provided in templated scripts for websites, socials, messages and telephone, we can also help to maximise awareness and engagement with a full suite of social media posts ready to release over the coming months. If you don’t have the time to post, or don’t feel confident in using social media, we can offer you support to do this via our social media managed service. Over 650 practices have chosen this option and if you’d like to see some reviews before you decide, head over to Practice Index.
If you book to join us, we’ll give you the discount code for the social media managed service so you can have 12 months for the price of 9 months at £349 for the year. That’s the equivalent of ½ day locum fee, or 1 week of admin time for a full year service. What’s not to like!
Looking forward to seeing the effects of this as a campaign to support General Practice. If you’d like to join us, get in touch hello@redmoorhealth.co.uk
A couple of years ago, a client came to us for help to understand the ‘digital maturity of their practices and PCNs’, asking us which indicators we would use to measure a baseline and monitor improvements, and then take practices through different levels of maturity. What a lovely question – we had a ponder in the team.
What was the problem they were trying to solve?
Well,
They knew they could access various digital data sets, but they couldn’t see a way to compare across practices, within PCNs, Boroughs or across the ICB.
They had to look in lots of different places to find data but couldn’t decide which elements would help.
Some data was open source but updated annually or with a time delay in release, so aligning and getting a baseline was challenging.
Some data didn’t seem to be relevant, but they weren’t sure if it was or not because they weren’t close enough to the service delivery to know if and how it helped.
Other data was behind barriers to access; usernames, logins, assigned to specific roles, and some data was provided to them directly by system suppliers.
They had programmes to deliver; online and video consulting, improve GP websites, advanced telephony.
They wanted to help their practices to mature, but didn’t know what ‘mature’ looked like.
They wanted to use data to underpin and evidence any improvement.
No small ask. My biggest fear was that anything we provided would be used to ‘performance manage’ practices who might appear at the ‘lower end of any scale’, without any understanding the complexity of primary care and running the risk of focussing on one dataset, in isolation of the others.
I’ve been on the receiving end of a ‘Red, Amber, Green rating’, and been given stretch targets in previous roles. Benchmarking can be a challenge and cause unintended consequences, if not communicated and managed well. It can be tough when working in one of the ‘top performing’ practices, then being compared against others who were given much less to ‘achieve’. I was very keen to stress that, yes, we could offer help, but the data we collated would come with a health warning about its purpose and use.
Roll on 2 years…..
We have moved through a process of days of data mining and cleansing via databases and working with multiple spreadsheet and worksheet merges. We’ve had people try and make it an easier process. We’ve seen the NHS develop further data sets and stop supplying some that were useful. We binned the idea of ‘levels of maturity’ as the improvements can fluctuate and its soul destroying to drop a level when working flat out. We have moved on to think more about how we visualise the baseline and show progress, whilst trying to make it as user friendly as possible, and finally, with the super team at Primary Care Analytics, ‘we’ve built a thing’ that people seem to be enthused by.
How Redmoor Health add value
This is the real gem for me. It’s not just about looking at the numbers, trends, or patterns, it’s about understanding the environment, each activity and then connecting the various datasets to tell the story for the people who are currently so overwhelmed with data and requests for how they can use it, they cannot see beyond the spreadsheets. We’ve had this experience this last few weeks, as a number of our clients are submitting their capacity and access improvement plans. Seeing the ICB variability of requests for plans, some helpfully pre-populated, others just big horrible spreadsheets, makes me weep.
Our team of primary care specialists can quickly look at the various elements in the Digital Maturity Index (DMI for short – because we love a three-letter acronym in the NHS) and walk you through:
How many people are enabled for Online Services? Average of 49% nationally
How many people are using online services each month? Average of 1.3% nationally for appointments.
How many people can order their medication online, then how many are doing this? Average of 49% are enabled, but only 12% ordering each month, in some areas its less than 1%.
The missed opportunity suddenly jumps out!
Many patients are keen to do things online, they understand how to do this, and want to help their practices by self serving. Some may have the NHS App, downloaded during Covid but are not utilising it to do even the most basic of transactions. Some have had a poor experience and dont use again. So, we can dig and ask why. It’s easy to spot those practices who aren’t offering online appointment booking and cancelling – but we take this a step further. We offer help with searches so they can see who has booked into the wrong slot – Yes, we all know about the patient who has booked their Asthma review online, but they’ve booked into a ‘smear’ slot. Practices may also be using a system that doesn’t feed into the ‘patient online’ data, that doesn’t mean they aren’t offering online booking. We coach and support ICBs to understand and check this, before making assumptions about performance.
We also help practices and PCNs to see where they may be creating some of their own demand and advise how to reduce this.
From a patient experience lens, we can view Friends and Family test data and GP Patient Survey data. We can look to compare patient experience and see the Telephony demand, lo and behold, 84% of calls are about appointments. We’ve already established that utilisation is low, compared to the patients ability to do this. We know how to help avoid the 8am rush and its not just about having cloud based telephony, its about call flow design, relationships with online services and good signposting to alternatives.
We have included electronic prescribing and repeat dispensing data, then we can compare pharmacy nomination and repeat dispensing to check that practices are taking advantage of these options to reduce workload demand.
We can look at the question: ‘how easy did the patient find the GP website to use’. If the website hasn’t got the right information about how to do things, it’s not a surprise that telephone demand is high. We can even see which services were used when the practice is closed, with 57% using NHS 111 nationally.
Already some of our clients are asking for extra data sets to be included, so we’ve added the Register with a GP Surgery data and the GP2GP data too.
Finally, we can look at how the practices in each PCN compare on a map and see patient satisfaction across a range of 8 questions, not just the 4 recommended in the latest Capacity and Access improvement plan requirements.
Not only does the DMI help us and our clients to see the opportunity, but it is also helps us to see the improvement of the practices using the Digital Journey Planner, our step by step coaching and knowledge system in use in over 1300 practices in England.
I’ve a couple of blogs whirling around my mind now, and knowing what to say and when to say it is often the thing that stops them from moving from my brain onto the paper (well virtual paper). I’m also a little unsure who would want to read too, but Coach Sharon says, ‘just put it out there and see what reaction you get’.
This week started off a bit challenging, as well as my main job at Redmoor Health, I still work in General Practice, and I was onsite at the surgery for the day. I had 3 tasks that have been niggling for a while, but I found each one so convoluted, I didn’t fully complete any of them. I was despondent and also fully understanding of why change in the NHS is flipping hard and takes time. So, I’ve decided to work backwards in sharing this week, as it most definitely ended on a high.
I’ve been lucky to go to Camp Digital for the last few years, hosted by Nexer Digital and as ever the speakers and people who attend inspire, uplift and confirm my hope that the start of my week’s challenges can be resolved with the right approach. There is a community of wonderful people, passionate about making things better, focussed on user research and digital transformation truly grounded in data, design, and experience. I hope some of them move into or stay in the NHS and not leave it, I hope others move to product suppliers and service design to build things better from the start. I also hope they have the opportunity and confidence to speak up and say, ‘this is too early to ship to market, we have more work to do’.
Having been in the workplace for 40 years this month, ‘improving’ is as much in my nature as is ‘sharing’. Work started for me in the nuclear industry with Quality Control, then Quality Assurance in 1983 and 1991, moving into the NHS 20 years ago with a stint in Service Improvement, then Commissioning and provision in General Practice. So James Plunkett’s keynote session was easy to relate to. James weaved his story of ‘history rhyming rather than repeating’ through the opportunity for scaling up and consistency, via Ford’s mass production, to making beautiful artisan loafs into the mass produced, square, white stodgy thing that many may think of as bread today. James absolutely recognised and rubber stamped the mantra that digital transformation is ‘all about the people and ways of working’, not just the tech. This is one of my favourite T-shirt slogans. Watching the NHS attempting to scale up, deliver consistency and increasing its awareness of quality improvement right now, feels like we are at a junction where we can go down the path of mass production, using methodologies and run charts, or, we can pause, and have QI in our minds as we ask curious questions to understand ‘what is the problem we are trying to solve?’, who’s involved, what are the issues, and then assess which approach can help. I’m minded to use the term ‘optimise’ a little less often now though James, but I loved this slide.
James presenting in front of his slide that is saying No, I will not build you an app hub thing with AI, ‘app’ and ‘hub ‘are both strikethrough text
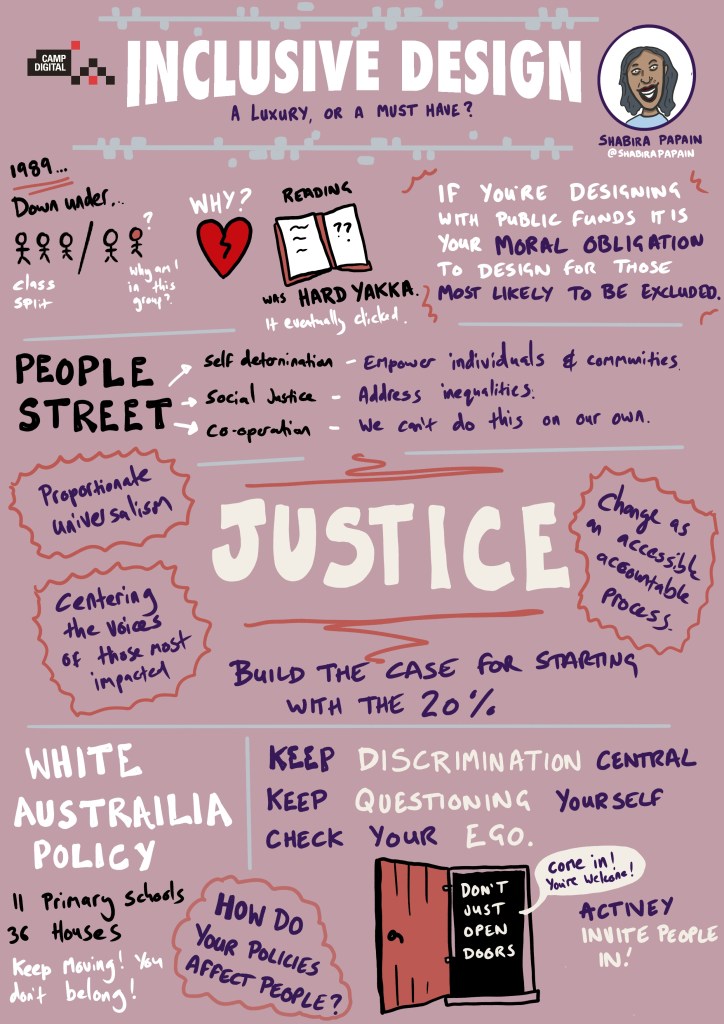
In the second keynote, Shabira Papain of People Street, shared her fun, obvious passion, and practical advice to explore social justice, and design for the 20% who are most likely to be digitally excluded. The NHS catchily refer to elements of this as Core20PLUS5.
Sketchnote by @ChrisSpalton
As public sector workers, we were challenged with the moral obligation to design for those who are excluded and not just to ‘open doors’ but to ‘invite people in’. This reminded me of earlier in the week, as I had just added ‘Register with a GP Surgery’ to our practice website, to help new patients register online instead of having to come into the practice and fill in a form (currently comprising 12 sides of A4 paper). Then our practice manager instinctively went a step further, got an iPad out of the cupboard (that’s another story), loaded up the site and showed the Receptionists how to help people who may be excluded from this new process, either because they don’t have devices, data or confidence to do this. Now, someone in the team can sit with people who need help to fill it in, rather than just signposting to the website. I didn’t need to mention ‘digital inclusion’ to her, even though it’s just one of the many priorities in the NHS. She knows her patients and how many of them still walk in for help and quickly offered an alternative support option. That is inviting them in, yes?
Next up, in a change of order, I decided on Elizabeth Buie’s talk ‘Older Adults: Are we really designing for our future selves?’
I’m (just) entering the category of ‘older people’, although as Elizabeth described, even agreement of who is old, offers variation in studies. I like to think I’m on the younger end of old. Wonderful, personal insights brought this session to life, with a bit of audience participation on who could hear (or not) the audio files linking age to changes in hearing capability. The best bit for me was understanding the difference between ‘fluid and crystallised intelligence’ as our ability to remember, learn and process may slow down, yet our knowledge from experience and education remains throughout life. I hear the term ‘subject matter expert’ often in the NHS and I’m sometimes asked in our team, to coach and pass on knowledge to our newer, younger colleagues. I also get to guide NHS commissioners on how to ‘deliver their priorities’ with general practice. But sharing 40 years of work in change, quality and improvement then knowing which bits are relevant, when to offer and who to, can’t quite be distilled onto an A4 product sheet, or a simple checklist. It’s much more nuanced. I know that the stuff I have experienced comes at random from my memory bank, whist I can forget in 5 mins what I’ve just been present in. Thank you, Elizabeth, for taking me back to the clicking keys of the typewriter and explaining why the ‘qwerty’ keyboard originated because the keys stuck on the most frequently used letters. Even though I know the order of an alphabet, car parking payment machines ordered by alphabet not qwerty, can raise my blood pressure!
Linking this to the workplace where we have the possibility to use voice to text software, yet we are still advocating training in touch typing for clinicians, seems like a missed opportunity. Thinking about dexterity, knowledge, and experience, then watching GPs who may have trained 30 years ago to quickly scan-read discharge letters for key pieces of information, seeing them struggle to navigate this same information in a variety of formats on multiple screens, seems a punishment we should address as a priority. Especially, if we are to improve the user experience of corresponding between healthcare providers. Watching people then retype (with errors) a summary of that information into another clinical system, slowly with two or three fingers is heart breaking, when many have used voice/dictation systems for years for their own letters, and the sending consultant in the hospital probably did the same. Even considering when a consultation is being spoken between patient and practitioner, then typed up rather than recorded as audio, or converted to data and narrative to meet the needs of data transfer, task allocation and patient information. There is a research project here for sure.
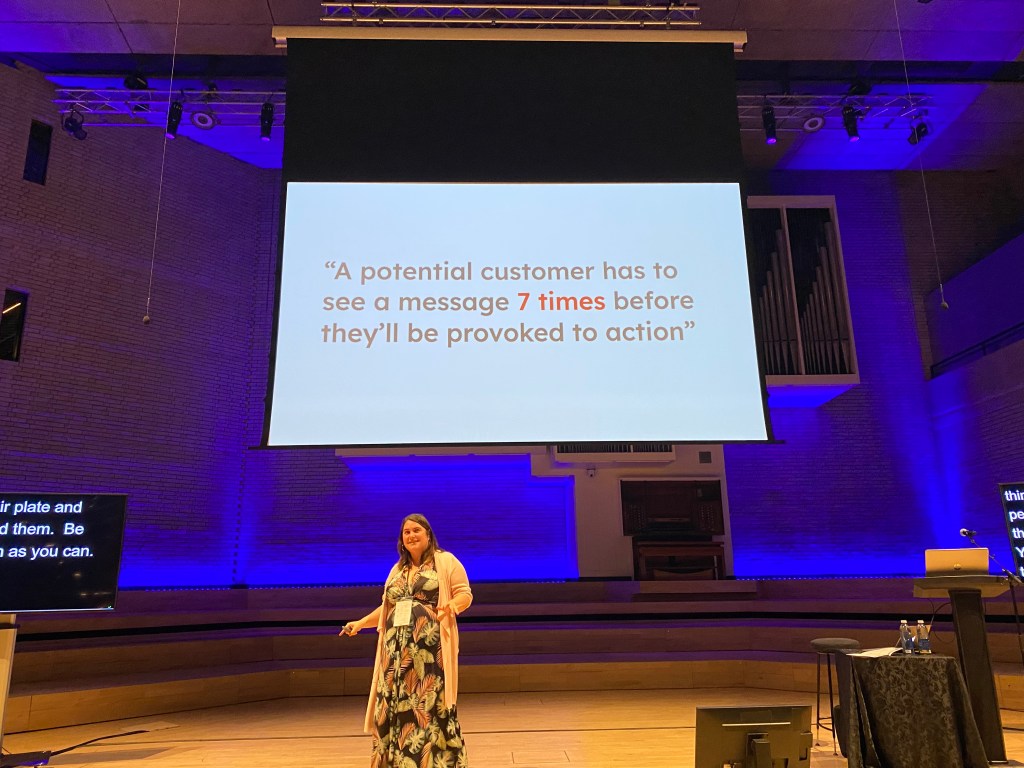
The afternoon sessions did not disappoint either. Audree Fletcher’s ‘Designing in the dark’ gave me many notes to take home, but this one message was a big one. A potential customer has to see a message 7 times before they’ll be provoked to action.
Audree reminded us that winning the big goals takes time, and finding the ways to achieve this is a lot more complex than just pitching your idea and hoping for the best. As someone who can get disheartened when others don’t just come with me, the hints and tips and final canvas gave practical suggestions to help. Understanding what else is going on in other peoples’ worlds, knowing the competition for funds, connecting the proposition to ‘what matters to them’, finding the right channels to drip feed the message, are all great ideas to get pitch over the line. I have loads of ideas how to make things better, then get dejected when they disappear into a dark NHS hole and layers of ‘commissioning by committee’. Meanwhile we lose months of progress whilst people ponder the relative value of this proposal over another. The NHS is amid yet another reorganisation, and many decision makers are involved in their own personal worlds of survival right now. Yes, I need to put myself in their shoes, but maybe it’s ok to also bring them out into the shoes of the people that they are supposed to be commissioning services for.
Example of using ChatGPT to explore bias associated in existing data, see the affects of pronouns he/she to same question, about who is working hard enough. @mmitchell_ai
Sarah Knowles and Lynn Laidlaw’s discussions of Data Feminism and challenging power along with where the patient sits in all this change, got a big thumbs up. As a sociologist, this talk touched my heart. Hearing Lynn question the ‘burden’ of healthcare and why it is considered as ‘work’ for practitioners but somehow described differently for patients, reminded me to challenge people with power, to acknowledge their privilege and share it out a bit more. Who has the power in the room should always be on our minds and it was great to see some familiar quotes and the effects of binaries, hierarchy and bias in our work.
The final keynote did not disappoint as data visualisation specialist Nadiah Bremer took us through constellations of data to rethink how we see connections. In amongst other more significant stuff, Nadiah represented the connections of google searches about cats and dogs in a beautiful way.
I’m watching some parts of the NHS gets it knickers in big knots over data right now, with an unhealthy focus on counting the wrong things and making erroneous connections. One attendee astutely observed that this final session, joined the dots across everything throughout the day together; research, experience, emotion, inclusion, context, power and data. Powerful stuff.
And so back to my earlier part of the week, I’ve managed to resolve some of the problems, but it still feels like I’m wading through treacle. I now better understand my new cloud hosted, telephone system call flow design, following a further phone call to the supplier. More edits are required to simplify for the user but still provide me with a whole load of data to understand.
My ‘Test patient’ for the NHS App, is no longer a Dummy patient, it’s a live Test patient in EMIS, even though I still can’t associate it with NHS App.
My Friends and Family data is now successfully uploaded into the bean counting system so we no longer have a big red mark against the practice, even though it’s an extremely crude mechanism to measure patient’s experience and I now have the 2023 General Practice patient survey to review.
For the people I work with in the NHS, you see this data stuff – we have a bit of a plan for you….watch this space.
And finally, although she may not realise it, I also get to take my sister to work.
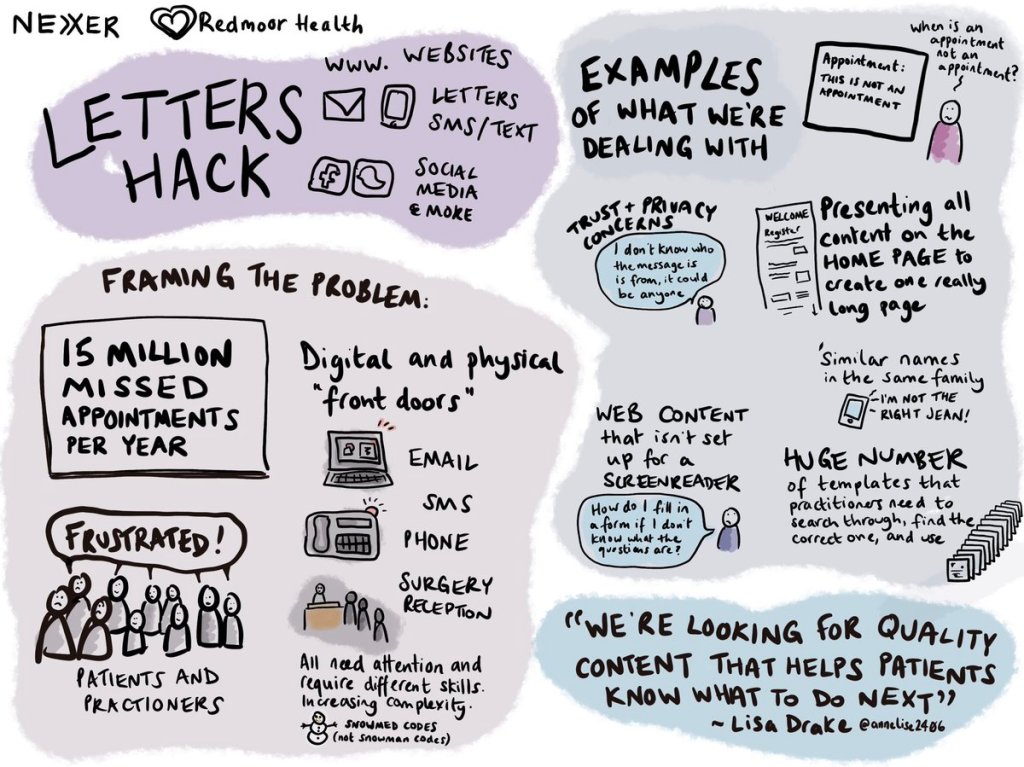
I’m a little late to the party with this blog, and others have already shared their thoughts and enthusiasm about #LettersHack – Rethinking patient correspondence (Eventbrite link for details) held on 12 Oct 22. If you’re curious to know what others enjoyed about the day, check Twitter and LinkedIn using the #LettersHack tag. Also, please do read the write up from Hilary Stephenson, MD, Nexer Digital, ‘Is there a Doctor in the room?
I wrote one of my first blog posts about improving patient communication and the opportunity to use digital solutions to improve patient experience in 2018, after a series of missed opportunities with appointments, cancellation, rebooking, transfers of information between health care providers, all which prompted me to share my experience. Four years on, it appears from the many examples of where it goes wrong, there is more complexity than ever.
#LettersHack planning started before the Covid19 pandemic, with a desire to improve letter content, so that users of health and care services would not miss vital healthcare appointments. Good patient communications help people to understand what has happened, what to expect next and feel included in their healthcare journey. As a result of the rapid expansion of remote modes of contact and service delivery, we extended the scope of the event to consider the multiple modes of communications now in use.
My part in the day was to set the scene for some of that rapid change in General Practice, but most importantly to state from the start; people don’t set out to do this badly and are often blissfully unaware of the consequences of poor communication. There are many constraints in the systems or software available to General Practice and this ‘stuff’ can make communicating it harder to do.
Many ‘internal thinking’ configuration choices were never envisaged to become visible externally to patients or other parts of healthcare. Electronic patient records weren’t designed with patient visibility as a factor, and we are seeing this very challenge played out now with concerns and delays to the online records access programme. I attempted to share some of these challenges; lack of time, poorly designed products, changes in regulation, societal norms and policy, and often, where the tech just hasn’t caught up. I offered plenty of examples of unintended consequences where communication just doesn’t achieve its aim, may have caused frustration, confusion, or concern, or just wasted people’s time.
At Redmoor Health, we feel passionate about supporting General Practice and offer lots of help and advice to front line teams to deal with these daily challenges. It was lovely to work with the Nexer team on this event, bringing their inclusivity and service design thinking to our digital communications and change, training and support programmes and we look forward to further events together.
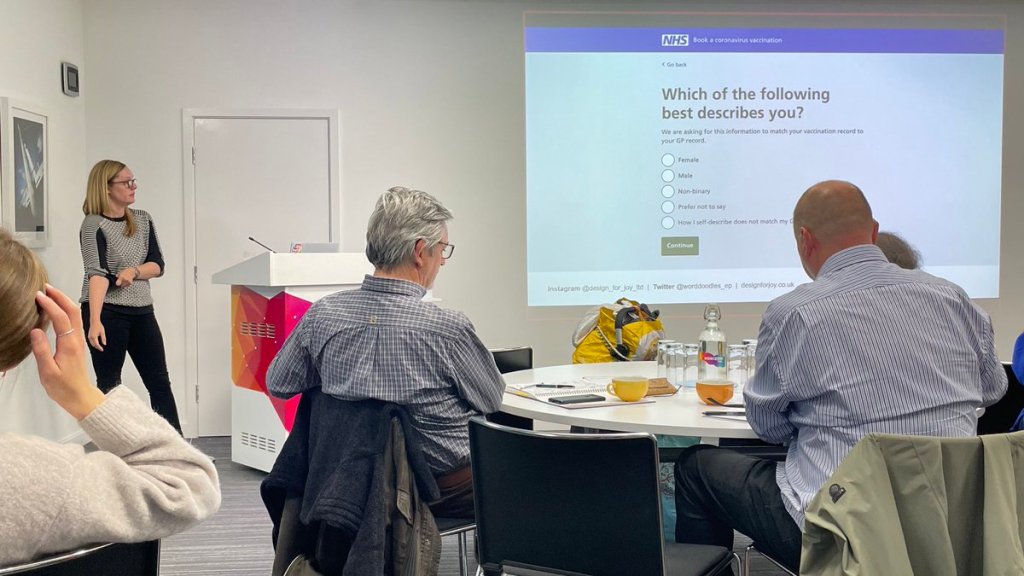
We all know the NHS is under extreme pressure, in fact someone commented in the session that ‘it’s broken’. At the same time, many of us are patients and active citizens who want to get this right and help where we can. There was definite sense in the room of ‘we can do this better’ without blame or criticism. In fact, Emma Parnell, Founder of Design for Joy, hit the nail on the head during her wonderful set, ‘Let’s talk about sex’ with the question, ‘How can we use our collective experience and influence to make a difference?’
Emma’s talk really drove home the absolute need for NHS services and systems to be inclusive, and the need also to question why we collect some data, along with how we do that in a way that makes people see themselves and feel comfortable accessing essential services.
Sarah Wilcox, Senior Content Designer, NHS Digital was equally inspiring, sharing her personal experience of less than effective communication (I’m being kind – the experience was rubbish) and walked us through the wonderful thing that is the NHS digital service manual, emphasising the importance of inclusive language to ensure broadest reach of the population, through the elements of the content style guide.
These were perfect examples of using our personal experiences to do something positive about it. The mix of people in the room provided us with an opportunity to consider many perspectives. Some offered insight into the setting of standards; core content requirements, timeliness of delivery of information, items that should be communicated between hospital and GP. Others, led strategic IT programs of delivery, such as covid vaccination invitations and vaccination recording. There were people who designed and delivered products to support General Practice with websites, communication and messaging systems, applications to access transactional services to help people order prescriptions, book and cancelling appointments. Most importantly, everyone felt aligned in their desire to improve the experience for users; and that’s people who both receive and deliver communications.
We chose to three main categories of communication to unpick;
Broadcast – using social media and websites
Targeted – using message systems to deliver public health campaigns
Personalised – using individually tailored content, via messages, letters, or even phone calls.
The afternoon breakout sessions had plenty of examples of communication to scrutinise and rethink or rewrite. Our group task was to consider ‘How do we use social media to maximise uptake of public health screening, whilst acknowledging the diverse communities we serve?’ We considered why people are nervous about some procedures, what they would want to know before attending, where we could find trusted information to back up short, impactful messages that reach the many different sections of the population. Fascinating discussion was held on what is and isn’t humour and plenty of chuckles about references to cats and dogs – even the Kama Sutra and a need for a modern etiquette guide to reflect today’s diversity – genius. We had rich, powerful, and engaging conversations that rarely happen over Teams meetings! We also realised that these events don’t work well as hybrid, our sincere apologies to the people at home who only got to see torsos, rather than faces due to camera angle.
Social media has great potential to reach diverse communities and many surgeries now take advantage of our support with public health campaign messages. Recognising time pressure, the Redmoor team help by creating content, administering pages, scheduling, and boosting posts to reach specific targeted audiences and have seen an increased reach and uptake of health screening as a result. If you’d like to know a bit more, check our social media managed service information.
When it comes to websites, and integration with online services and consulting, we can also help NHS Teams and practices to smooth that patient or user journey, so that the practice and patients gets the best out of whatever system is available to them. We’ve created digital journey planner to help staff to self assess their digital service delivery. Three modules are already available to support good patient communication, GP online services and digital inclusion, with lots of learning materials to inform about websites, inclusive communications, effective use of messages etc.
Over the coming months, Nexer will continue to gather examples of patient communications, good and not so good on their airtable platform in the hope of creating good content library and guides in future sessions. Iatro also have a commons library to share good website content for GP Practices. Drop yours in via any of the social media platforms with #LettersHack tag and we’ll pick them up.
I can’t wait for the next session. Thank you to everyone who joined and made it so good.
PS Hilary did tell everyone we are sisters; I’d have let people guess….
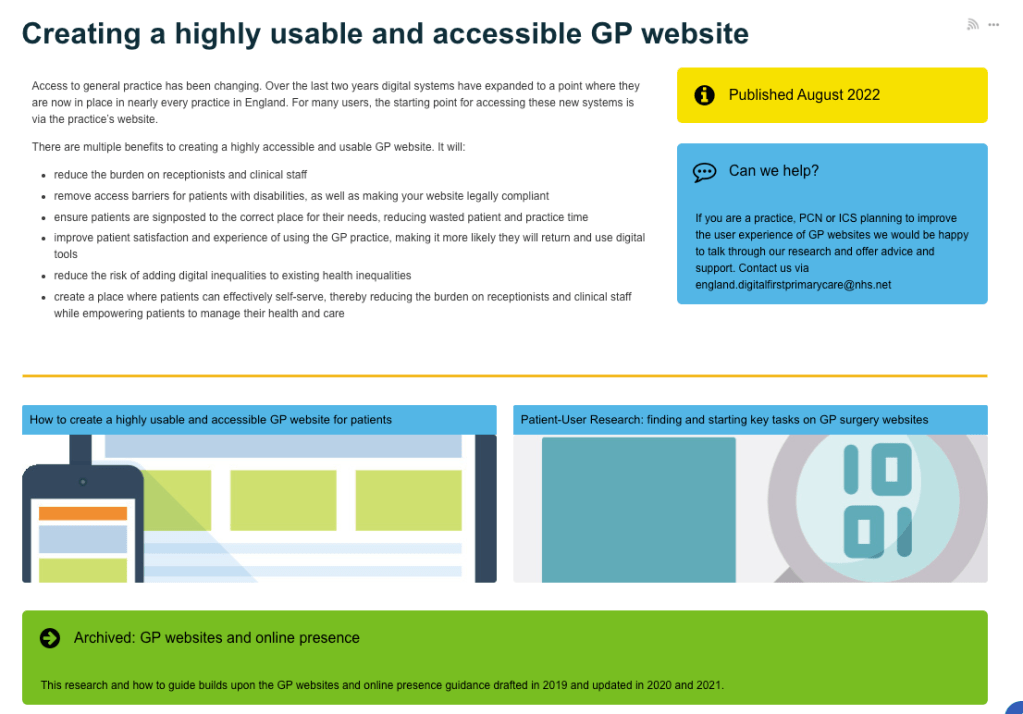
Future NHS page with the ‘creating a highly usable and accessible GP Website for patients’ guide, and ‘Patient-user research to support’
In the last few weeks there are some super updates to the guidance from NHS Digital and NHS England that will help GP practices to create inclusive content and usable websites. It should also make lives easier for people who need to use the ‘Digital front door’, aka GP practice websites.
You’ll realise that I have a bit of thing for GP websites. In my day job, I sit at the intersection between policy makers, NHS commissioners, specialists in inclusive and accessible research and service design, product suppliers and the people in practices who try and make sense of it all, to provide services to us as patients in the NHS. It’s a nice place to sit. I don’t need to be a specialist, I don’t need to have the technical know-how, and although I do know a fair bit about General Practice, service improvement and delivery, we all have experiences as patients that we can lean on and learn from. This guidance brings much of that knowledge into one place.
This is why the guides are so helpful….
GP Practices have a myriad of contract requirements to meet, in fact there are 10 pages of items listed in the ‘highly usable website guide’. Many of them are iterations of earlier contract requirements, it’s no wonder practice teams are confused – I’m confused by much of it too. The GP website supplier market is large, as is the online consultation market and each supplier clearly wants to do the best for their clients – the practices. But occasionally and possibly due to the market competition, these suppliers sometimes focus a bit too much on their own branding and product and not quite enough on the usability of their product, either from a General Practice team perspective or the intended end user, i.e. the patient. They may forget that their product needs to be connected to another NHS service and so needs to conform to the standards and style of the NHS brand, which is trusted and researched to reach as many people as possible. Often, the user is confused when they access information online and get diverted off to a supplier’s platform, or suddenly the page no longer looks like their GP practice or even an NHS service.
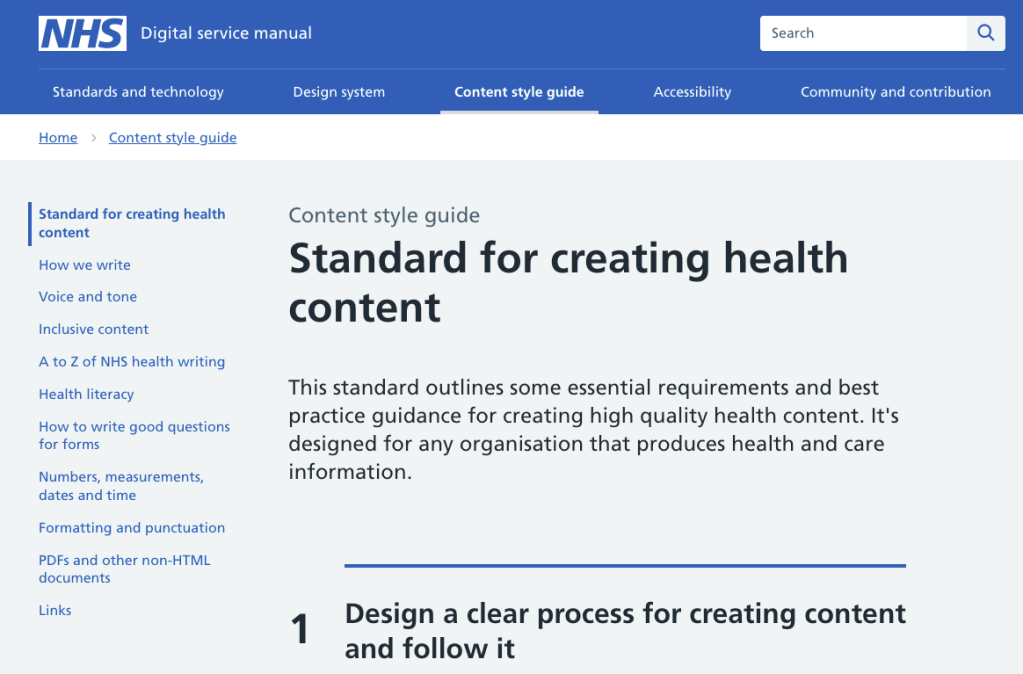
Home page from NHS Digital service manual showing the Standard for creating health content
Colours matter, language and content matters, the user’s journey matters, the technical layout matters. For the practice teams who have a million other things to do, simple ‘how to’ instructions and examples help enormously and these guides offer sample layouts with ‘things to include’ and just as importantly, things ‘not to include and say’.
Hilary Stephenson, Managing Director at Nexer Digital says,
‘It’s great to see the convergence of user centred design standards and technical platforms across the NHS and their vendor network. Sadly, in our work we have seen real issues with the core usability and accessibility of websites, consultation platforms and apps used for digital engagement. This feels like such a missed opportunity at a time where digital inclusion is vital for patients, their families and those delivering services under immense pressure. Anything that provides practical guidance, which is evidenced by user research and makes things more inclusive, from content design through to platform configuration, will improve the experience for patients, clinicians and administrative teams.’
Hilary Stephenson, Managing Director at Nexer Digital
Now the work starts….
There are over 6500 GP practices in England, just over 900 in Scotland, almost 400 in Wales and over 300 in Northern Ireland, each serving their average registered population of 9000 people. That’s a lot of people to reach to reduce the variation of experience for users and for practice teams who provide information. We have incorporated this guidance along with simple advice, hints and tips into an easy-to-use system called the Digital journey planner (DJP). The first module; Patient Communications deals with Websites, Social Media and Messaging, The second module; GP Online Services covers everything that practice teams need to know to provide a good online service and make that easy for patients to use. If you are getting ready for patients having full online access to their medical records later this year, it’s a must. Our next module, due for release at end of Sept will be Digital Inclusion.
Map showing location of practices in England using the Digital Journey Planner. Blue dots have Foundation access, green dots are practices with Enhanced support from Redmoor Health to embed digital service delivery. Aug 2022.
So far 10% of practices are using this system in England currently and we aim for 25% before the end of the year. At Redmoor Health we work with practice teams to help improve digital knowledge, skills, confidence and competence and offer support in terms of training, coaching, advice and share best practice resources that save practices time when searching for help. These guides are essential learning tools to embed in the DJP, so they are easy to find and stand alongside practical hints and tips when to use. Some areas have already commissioned Redmoor Health to carry out reviews across all their practice websites, just to get a feel for the scale of the problem and ideas how to help. Others have offered incentive schemes for practices to have the time and space to make the changes, so we anticipate this as a big opportunity to improve, standardise and simplify access to information.
The suppliers….
Good suppliers have been using these standards for some time and have already created NHS style guided website templates, that meet the accessibility and usability needs of users and practice teams. Others recognise that they need to encourage practices to move away from old legacy systems, personalised styles and ‘whizzy websites’ to be more consistent, and to simplify the user journey. I’m quite sure many more will now take on these recommendations following the detailed patient user research that informed the guide. I spoke to a few to get their views of the research and guidance.
Iatro Practice 365 have already produced a simple version and template for practice teams to know what to add to their website. Thomas Porteus said,
‘We’ve been behind the NHS Service Design Toolkit since we started, it’s been a pleasure to work with NHS teams openly and to be able to contribute our own code back to the project for the good of all NHS organisations. The guidance is a really great point of reference for practices wondering where to start, and what to avoid’
“As advocates for patient-friendly, accessible websites since we began working with GP surgeries in 2004, we warmly welcome this new evidence-based guidance from the NHS Digital First Primary Care team. Clearly focused on simplifying the patient journey, the guidance offers practical advice and tips for practices and commissioners aiming to improve patient experience, reduce digital inequalities and remove barriers to access for patients with disabilities.“
‘At Livi we welcome this new guidance from NHS England. Accessibility is not about sticking assistive technology onto the website. It is about building the website from the ground up to work with third-party assistive technology (e.g. screen readers). It is also about ensuring the website content is written in a way that is clear and understandable by the majority of users. By using the NHS Digital Service design system, Livi websites are NHS branded, optimising functionality and providing confidence for patients to engage with online GP services (as well as other locally commissioned services and third-party tools). We believe practices should have generic accessible content and definitions of local service providers to help patients manage their own care. This approach has allowed us to build a practice website platform that gives practices back more time to spend on patient care by:
nudging more patients to digital services and appropriate alternative NHS services,
reducing the time needed to manage and maintain the website
Dillon Sykes, NHS Partnerships Manager
To the commissioners – let’s do this together….
Most useful in the website guide is valuable information for NHS commissioning teams to help procure GP websites ‘at scale’ and to know what to ask of suppliers in terms of user testing. Perhaps now is the time to rethink the stance that ‘it’s a GMS requirement to have an online presence’. This must be the way forward to support local population communications and connecting the services at a local level for patients. It will support primary care network development and reduce the burden on individual practices to know and learn about website technicalities, so they can just focus on the message and how it is presented or accessed. As more services are delivered together, why would we expect each separate practice to upload its own content and service description? Surely this is done once by the local service provider? Let’s take a current example. Practices will all be delivering Flu and Covid boosters soon. They need one single page for who’s eligible, then the ability to edit and add what’s happening locally, so that people know how to book and where to go. Currently each website supplier may duplicate this, and some are good enough to offer a ‘Flu’ content page. NHS England have issued the criteria in a Specification. Public Health (UK Health Security Agency) have some promotional material, and poor practice managers will be trying to make sense of it all to tell their patients what is happening, whilst awaiting the final dates from vaccine suppliers and working out which members of the team can deliver. One forward thinking area has thankfully collated all of this information together for its member practices and wait for it…… shared it as a google drive document to 200+ practices via email!!! That’s my Friday job folks – to upload and create this years Flu page.
google drive document containing all of the information required for 2022/23 Flu campaign
Hopefully, you can see where I’m going with this. Do we really need 6500 individual digital front doors? I think not, but always open to be persuaded if you think the status quo is better.