It’s been a whole year since I last blogged. And it’s been a funny year at that. If you read my last blog post, it was all about the expectation of change, moving home, working less, trying to get fitter. Best laid plans, as they say.
The house we were buying on Islay fell through; it obviously wasn’t meant to be our dream home, but I hear that Janet Street Porter is interested, so there’s a claim to fame at a quiz. Having sold up with nowhere to go, we embraced the situation. With our belongings in storage, we were fortunate enough to have a lovely few months as houseguests with family, interspersed with an odd Airbnb here and there, whilst we searched the property market and visited places to find our next home.
I’ve watched many home renovation programmes over the years, and still felt like I had the energy for another project, so talked Mr D into a little ‘doer-upper’ on Kintyre, where we moved to in July. We are surrounded by fab beaches and ferries (when they are running!). It’s remote, but still near enough to civilisation and I can watch the ferry over to Islay when up out on the hill with dogs.
We are still waiting to start a renovation that seems to be taking ages, so I’ve swapped the joy of dealing with estate agents and solicitors for planners and architects; I just can’t seem to avoid dealing with ‘Professions’.
The end point is Grand Designs meets Scotland’s Home of the Year (in my head). However, the reality of some elements feels unsettlingly similar. I should have realised when the septic tank collapsed in our first month that it wasn’t going to be plain sailing. I didn’t think anyone could get excited about a digger and a concrete tank, but there you go, it was the highlight of September, while we waited for planning permission to be approved.
Things got a bit sticky healthwise in the Autumn, when I experienced Scotland’s NHS system as a patient, not as an employee or advisor, as I might have planned. After spending too many years sitting at a screen, my back decided to shout about it and remind me to move more. I couldn’t help but have an interest in looking at the Dr.’s screen. Vision seems so small and cluttered – I could do a lot with that. And no NHS App up here – what’s that about Scotland – I’m dying to help with that too. We chatted about access, remote diagnostics, support for Primary care, and for the medics out there, a few X-rays and scans later showed up usual aging osteoarthritis along with Cam hip impingement, osteophytes, facet joint degeneration, and a nice little slip of L4/L5 – painful!
Time to take control of your health, Lisa!
With daily (who am I kidding) TaiChi with Dr. Potts, a regular massage with Jacqui B,and Pilates in a class and 1-1 with Kath at Headingly Pilates, things have improved enormously. It all felt a bit self-indulgent for someone who isn’t used to putting themselves first, but I know and now feel the importance of keeping active, and these regular sessions are scheduled maintenance for the body. I did wonder, though, if I’d stepped into a scene from 50 Shades of Grey when I first saw the Pilates equipment…..
I even signed up for a winter Pilates retreat at Torrisdale castle, ending up in the Kilbrannan Sound on 1st Feb, in 6 deg water temperature and no wetsuit. A lifetime experience as a Dolphin jumped out of the water, just before we entered.
To balance all this so-called ‘leisure-time,’ I’ve still been helping out at Redmoor Health and with my role in the NHS at the practice.
In the New Year, we were straight into migrating clinical systems, moving from EMIS to Medicus in mid January. Following on as the 3rd EMIS practice to migrate, but as the first in our ICB, many things were still a ‘first’, so it does feel like we are paving the way for others. I’ve got right back into product development, and it’s made me realise that’s where I can help out most. That sweet spot between the product team, service provider, patient experience, and stakeholder relationships.
Whilst I love this sort of work, I’ve enjoyed the freedom to be out in the fresh air when I want to be. I’ve valued that balance of home-work-life this year and need to do more of it. So, today is my last day at Redmoor Health, after 8 years with the Company and enjoying a great chapter in my career. I’ll still be around for their Advisory Board, having watched and been part of the company that’s grown from a team of just 5.
As Spring approaches, I’m not retiring though, just turning over a new leaf.
As we approach the end of the first quarter of a new Government, I’m taking a moment to reflect on a few papers and articles released and considering these against my experience of trying to use and implement Digital in the NHS.
I’m sure many of you will have seen or commented on the recent paper ‘Preparing the NHS for the AI Era: A Digital Health Record for Every Citizen’, as part of the Future of Britain policy initiatives. As usual, it was met with the full range of commentary, from enthusiasm and welcome support to the obligatory dumbing down headline about ‘chatbots doctors’. Dr Charlotte Refsum, Director of Health Policy, Tony Blair Institute for Global Change summarises the key points in her LinkedIn post (which is where most of my blog readers get their information these days since the demise of X – but that’s another story!)
Please can we fix the basic requirements first?
I totally understand the response: ‘Please can we fix the basic requirements first’. One of the biggest surprises when I joined the NHS 20+ years ago, was that the basic user requirements for tech were at least 5-10 years behind the nuclear industry that I had worked in previously. I recall being astounded at having to submit a business case for a £250 desktop multi-function printer/scanner to save hours standing at a photocopier, printing patient records, then re-typing that information into templates to be sent by email, and then yes, posting the paper records to the PCT HQ. My request didn’t get approved – I moved on.
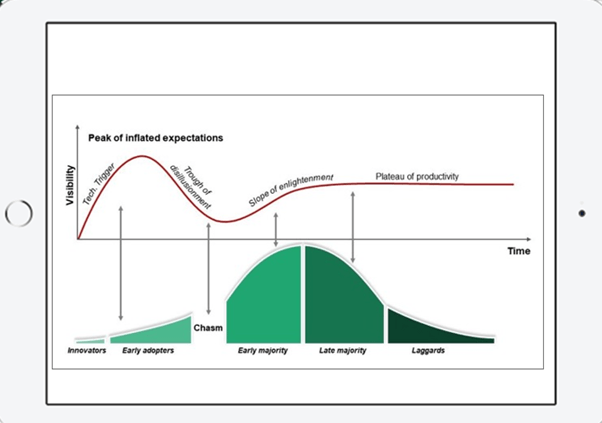
During those 20 years, we have seen variable improvements, some big-scale projects start, get delayed and then scrapped, and a lot of money paid for products not used. I use this image regularly in my presentations and it feels like the gap between the early adopters and laggards seems to be widening, as well as the hype increasing, quickly followed by the trough of disillusionment. I still take part in video meetings with practice teams, all huddled around one PC. No spider phone, or owl camera in the meeting rooms, and some don’t even have a webcam and headset to participate fully.
The Citizens Digital Health Record (DHR) and Primary/Secondary Care interface
I’ve been an advocate of patients having access to their full medical records for 10+ years since I worked in practice and could see the value to patients as well as to our workload. However, creating a new multi-sector DHR in light of the legitimate concerns around procurement and data security is not without challenges. Seeing the attempts to share and view patient data across health systems has been soul-destroying in some instances. The requirements of PCARP – ‘cutting bureaucracy’ and addressing the challenges of the primary/secondary care interface seem to be thorny too, with the bureaucratic referral process incorporated in the BMA collective action guidance. As a Commissioner in Cumbria in 2008 looking at part of this work, I recall a discussion with an Orthopaedic consultant defining the pre-surgery baseline test information they required. I asked why Primary Care couldn’t just create and supply a ‘view’ from the relevant part of the GP clinical system to Secondary Care. It has been technically possible for some time, but still not done. I still see each ICB or Region reinventing this wheel or worse, not addressing this issue at all.
The Technology Innovation Framework ‘new market entrant’ clinical system suppliers are still building functionality to send and receive ‘documents’ into and out of hospitals because they have to design the new systems to ‘fit’ with existing NHS systems and workflow. Secretaries spend hours listening to digital audio recordings and populating templates, administrators uploading or archiving the same, all to ensure the correct coded data is sent from A to B, or to make sure payments can be attributed for the work. This is light years behind where it needs to be in thinking and design. Why are they not designing these new systems to allow secure structured data flow and visibility, separated from ‘task handovers’, with a ‘patient friendly’ version alongside? I’m sure many of us have looked at our records in the NHS App and wondered what on earth some bits of it mean. So now, I’d say that people need access to their ‘health information’, not their ‘medical records’ – its subtly different. Clinicians need medical information in order to advise or treat, Managers need a different set again. Transferring care, is different from the information that patients need, as is the need to track flow of activity for demand, capacity and resourcing, and then capturing outcome data to check that the intervention works. It surely cant all sit in one DHR, can it?
Lord Darzi’s review
There will be many that comment on yesterday’s release of the Independent investigation of the National Health Service in England, AKA the Darzi review, for many it contains no surprises. This review along with numerous papers and articles all feature Tech or ‘Digital, not Analogue’, and AI as a central part of the solution. Those of us involved with change, implementation, and optimisation know, that the Tech alone will not suffice. Having the headspace to think differently, when you’re up against the clock, or burning out so you can’t even consider taking the risk of doing something new, all needs to be factored in alongside the Tech. Let alone addressing the working across silos.
Exhilarating and terrifying – not just the internet, but AI
Then I came across this old clip of David Bowie predicting the impact of the internet in 1999 and I have to say, I can have similar feelings about AI – it’s both ‘exhilarating and terrifying’ at the same time. I can get enthusiastic when I have a call like the one I’ve just had about predictive analytics, taking millions of data points and using AI to understand the trends. At the other end of this, I do more than roll my eyes when I see glib predictions that AI will solve all our problems, or replace the need for people, or be the only source of the truth.
Having worked with patient and staff data, and understanding the requirements of data controllership, the risk of data breaches seems a priority, closely aligned with clinical safety and acknowledging bias in all its forms. All the marketing hype is about efficiency, so it is great to see sensible guidance being released.
As the system strives to move more and more services to digital platforms, leaving people behind, who may already be digitally excluded and suffer poorer health outcomes as a consequence, is equally important. Nexer Digital offers practical service design advice in this blog post by Chris Bush; AI for all; Inclusive design principles for the use on AI in the Public Sector and Danny Lancaster offers us real-world use cases to help us consider how AI tools can support a more inclusive workplace, not just a more efficient one.
So, with all of this in mind, we’ve decided to get the experts in the room and see how we can solve some of the core General Practice problems, using AI safely, inclusively, and effectively. When we asked people to tell us what problems they like addressed, it’s the mundane, repetitive, time-consuming things, not the boundary-pushing stuff.
If you’d like to join us at our Custom GPT Hackathon on 3rd Oct in Leeds, to learn, share knowledge, and maybe enjoy a pizza even whilst having fun, why not come along and find out which side of the David Bowie ‘AI line in the sand’ you’re on?
Meanwhile, I’m leaving you with an image of Dr Keith Grimes, staying up all night testing the new ChatGPT models in preparation.
Getting the best out of remote and digital general practice
Some of you will know I live in beautiful scenic Cumbria. So, you’ll have an understanding all about lack of public transport and how flipping hard it is to get anywhere in a hurry.
Some of you will also know that I have a touch of FOMO, so when I get an invite to two things at the same time, I struggle to decide and often think, maybe I can do both.
The dilemma
Our Redmoor team were having a redesign session on 24th April, partly in response to some NHS contract changes, partly because we’re 12month into one programme and 3years into another and we wanted to reflect. Also, because we want to look forward and make sure that our products and services support a hugely stressed system in General Practice, and we have the expertise in the team to help.
Then, I get this invite to an event presenting the findings of quality research by the teams at Oxford, Plymouth and the Nuffield Trust, delivered in the House of Commons, for MPs to listen in order to understand the issues and complexity of modern general practice remote care. The research team have created this summary to share, so that others can learn from the 2-year study and build the findings into their work.
I’ve been involved on the edges, as part of the expert advisory group and as a participant in a series of workshops, but this is very much part of my everyday work and something I’ve been passionate about in the NHS for many years. How could I turn that invite down.
I decided to attempt to do both sessions. One from the train, the other in person.
Plan for the unexpected
What I didn’t plan for was a horse event, total disruption to the road network, and it being ‘surgery day’ at the House of Commons, resulting in the longest queue to get in, the fastest transit through the building and security, and arriving just slightly late for the session (along with three others, reassuringly – I wasn’t the only person who mis-planned). For those expecting selfies with the Ministers – no time for that I’m afraid.
The event in person
During the presentation, hearing the personal stories of those affected by ‘Remote by Default’, as receivers and providers of services, will always bring you down to earth, irrespective of the magnitude of the setting.
Professor Trish Greenhalgh and Dr Emma Ladds sharing some of the experiences from the research
The strongest message I heard is that people need and value continuity of care to get the most from the experience, prioritised over quick ‘transactional’ access. Secondly, that delivering and receiving care remotely (telephone, online, video, asynchronously) can be safe (see Table, p10) but that training and developing the right culture is as fragmented as the technology used to deliver care. Thirdly, that the purchasing of technology is not just about the product, but the variability of its implementation has resulted in unequal impact (see my other blogposts). Finally, that although the NHS has plans to embed this into education, it will take a long time, and General Practice need the help now.
So, the training needs and competency framework are super helpful, and for those supporting general practice this research is gold dust, as it should inform the basis of any training and advice.
We’ve already used this patient facing communication created by the researchers and posted out a social media campaign across 700+ practices to over 30k patients to inform and encourage people to access care this way.
How to get the most from
Although it was a flying visit, I met and hugged some incredible people that I’ve only ever seen on screen or interacted over socials. I sat beside someone who also hailed from the North and it transpired that I knew their father – how Cumbrian is that!
What happens next
The research team are sharing their learning on a public zoom event on 22nd May, so watch out for details if you’d like to join us.
The event from the train
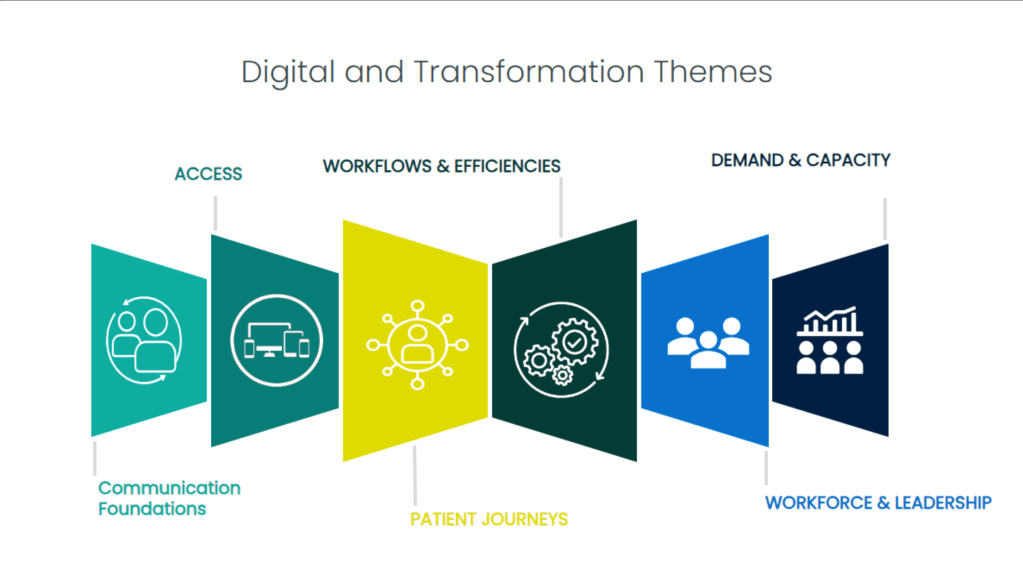
Back at the Redmoor office, the team had a successful day too and now have a clear plan for our digital and transformation products and services, so watch out over the coming weeks/months for updates.
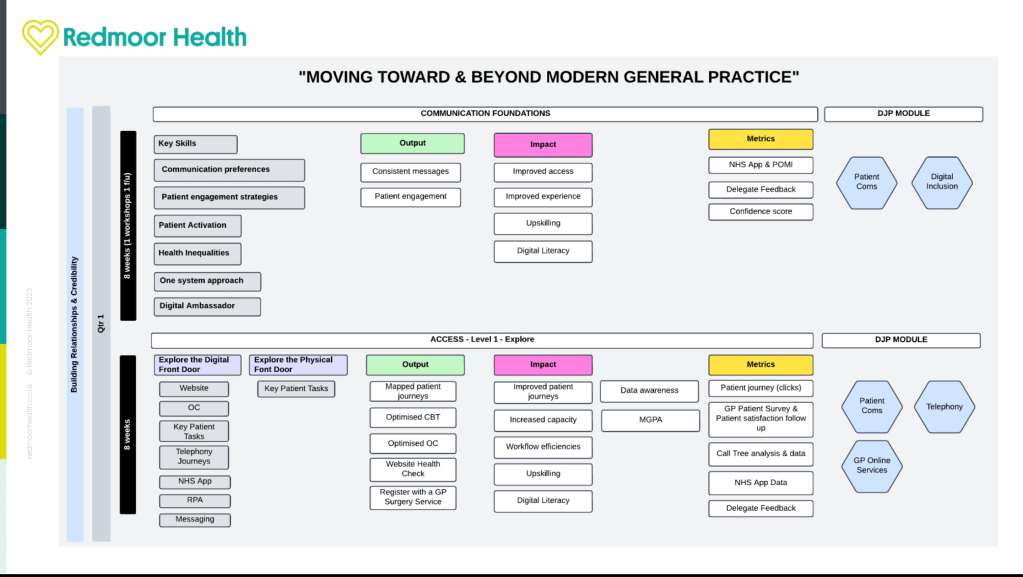
We took part in our joint HSJ Awards - Best Consultancy Partnerships interview with one of our clients this week, as we come towards the end of a 3-year programme. As one of the original gang at Redmoor Health, it was nice for me to reflect on the successes of a strong relationship, developed to deliver a long, multi project programme aimed at increasing digital access, improving patient communications, upskilling the workforce and supporting the Digital First team to deliver their aims. I took a moment to consider this strategic partnership against the current climate of change and chaos in Primary care and thought I’d share some musings with you. BTW, its 8mins long so get yourself a brew and ponder with me.
Finances
Its that’s time of year, when in the last quarter, there is traditionally a frenzy of activity in General Practice. Teams are chasing patients and are working hard to recoup any finances earned throughout the year to maximize payments, following delivery through QOF and the Primary Care Network contract. With only 7 weeks to go to the new financial year, uncertainty over pay and contract negotiations is making next year’s planning harder than usual.
Throughout 2023, there was a raft of new guidance, contract and service changes that managers needed to understand. ICBs and Regions are now comparing progress against targets and seeking assurance or evidence of improvements against new criteria before they can release payments. Some are excelling at this, others finding it hard work. That’s on top of the usual round of ‘heck, we have to spend this money before year end’ last minute decisions. Previously, we’d agree with our clients to receive and hold this year’s £s, then together work up a more detailed scope for delivery into the new financial year, when their priorities are a bit clearer and they can engage properly when primary care have more time. With the reorganisation and requirement for a 30% reduction in costs across NHS Regions and ICBs, some people are facing redundancy or moves to other jobs, consequentially, loss of local organisational knowledge and decision-making inertia is becoming clear. Also, the combining of primary care transformation and digital budgets is affecting financial flows and prioritisation of projects. Clawbacks on unspent budgets are being mentioned in dark corridors and on socials, which is a sad reflection both on the plans and especially when primary care need the funding right now.
Primary care contracts
One element of the PCN contract is the capacity access and improvement payment. Unsurprisingly (clue is in the name) this is largely about improving patients experience and access, with payments linked to improved appointment recording. As part of our Digital Managed Service, our team have been supporting PCNs to deliver this guidance, contract changes and ‘new models of care’, so my super colleague Dillon Sykes and I thought this might be a topic for discussion at our session at Best Practice, London on 28 & 29th February. We’ll explore some of the headlines, overlaps and gaps, ponder a little around the various checklists and criteria to be met, then hopefully share some practical steps to help.
We are seeing lots of angst that the General Practice Appointment Data (GPAD) dashboard still seems to contain inaccuracies and a lack of clarity over what is counted, and how to make historic changes etc that will impact on payments. New to the ‘additional roles’ stables are the Digital &Transformation Leads and alongside PCN Managers, both are still trying to understand appointment mapping guidance released in 2021. Clinical system providers have released workarounds in the last couple of months as temporary fixes. Frustrations are appearing between General Practice and PCNs as the data is held and configured at practice level, but the impact is felt in the PCN.
It’s great to hear that some ICBs are supporting well, providing datasets throughout the year to keep an eye on progress. We are sincerely hoping that ICBs take a pragmatic approach to releasing the final 30% payment, whilst the data is still ‘more than a bit flaky’ (technical term).
To help with GPAD, our team ran webinars and held 1-1 sessions with practices or new D&T Leads to go through their configuration and data. We produced a simple GPAD tool to help navigate the guidance and we’ve also asked passed on quite a few questions to people in NHSD/E to gain clarity.
Procurement of new digital solutions
This last year’s quarter is also a little bit different though, for many suppliers of services and products to the NHS. It’s not unusual for slippage in the NHS, but some of the key elements of the Delivery plan for recovering access to primary care that slipped or were reprioritised, will have knock-on consequences for many colleagues in the product and supplier landscape. This will also affect practice teams and inevitably, on patient services.
I’m fortunate to occasionally take part in user research and know the NHS team are working hard to make the experience of the buying catalogue better, but this delay has impacted on ICBs, PCNs, Practices, Product suppliers and support organisations like Redmoor. Part of my job is to seek out new partnerships and products that will help to improve General Practice, and I love chatting with new suppliers to find out how their solution will help. There are a few with products that will knock your socks off but are not available to purchase from the existing procurement frameworks. Some PCNs are bravely buying directly, as they can already see the value, but many are nervous or don’t have the finances to buy direct, especially if their local ICB is expected to and will fund (or even part fund), once the new buying catalogue is available.
As a consequence of the delay, it looks like many commissioners have little choice but to extend existing digital solution contracts for another year. This can leave practices with products that they didn’t choose or don’t use and patients don’t like to use, so stick with the conventional methods of access (Telephone). So, in ‘kicking the can down the road’, existing suppliers breathe a sigh of relief and new products don’t get into the market, leaving us all feeling just a little bit frustrated at what might have been for another year. Do we invest time and energy trying to optimise solutions that we know don’t fit the needs of our staff and patients?
Our new procurement support service logo
Suppliers tell me they have lots of interest from ICBs and PCNs but can’t recruit to scale up delivery until they know the contracts have landed. There will be a rush at the end, and we know deployment and implementation will suffer. These tools are essential to deliver high quality 21st century primary care. Having been through this process with one of our strategic clients last year, we have experience and are well positioned to support suppliers and ICBs with market and practice engagement, early implementation, adoption and spread. So, if you want to plan early, drop us a line and we’ll walk you through how we can help.
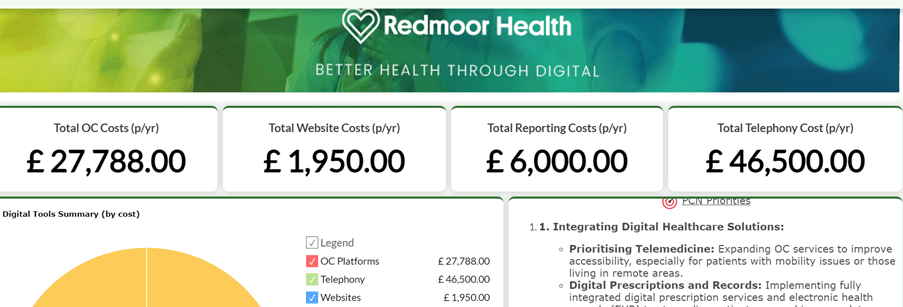
An example PCN dashboard showing the costs and variation of products in use.
Research
In addition to user research for products, I also contribute to research for new services in development and I’m delighted that NHS are developing a guide to improving messaging. This has become such a complex area, since the inclusion of messaging as a requirement for all online consulting tools. The NHS is paying twice for quite a few functionalities and the holy grail for practices was always to have digital solutions in just one platform. There are a couple of suppliers doing this extremely well, and with the increasing desire to reduce SMS costs, data messaging is the way forward for many. One super research project that I’ve had a small involvement as part of their Expert Advisory Group is the Remote by Default project from the teams at University of Oxford and Nuffield Department of Primary Care Health Sciences. They’ve released some great resources following a 2 year study into remote care. We’ll be helping to push these out to patients in over 700 practices via our Social Media managed service, and will build the training competencies into our programmes, so we are confident that our work is grounded in rich research. What is interesting, is the different approaches across the Nations. Scotland have procured one video consulting platform for the whole nation to use, with a contract to 2026. This means they have one set of patient facing resources and one training platform for all practices and users. Very different to our market place approach in England and probably a lot less confusing.
Now – lets’ talk telephones
As another example of what I’ve just described in the procurement section, lets have a look at the requirement for Advanced Cloud Based Telephony. Seen by some as the panacea to ‘the 8am rush’ and made a requirement in the GP Contract by end of 2025. The Better Purchasing Framework was issued, some ICBs took advice and started to plan the ‘at scale approach’, working out whole system requirements, engaging with practices and PCNs to gain advantages of greater purchasing power, optimise local infrastructure and achieve some consistency of service offer – great stuff! Then a letter appeared late Nov, expecting all practices to sign up by 15th Dec 2023 or they would miss out on the funding opportunity. Thankfully, someone realised the well-earned Christmas and New Year holiday was looming and the deadline to select a supplier was moved to 15 January 2024, with a signed contract by 2 February 2024 and go-live by 25 March 2024, with all features in place by April 2024 at the latest. Just another added pressure in the last quarter of the year.
Now there is anxiety over where the costs will land, and we had a flurry of requests to help people make a choice urgently, so they didn’t lose out on funding. We had others that had already moved to cloud telephony before the contract requirement was released, but had chosen suppliers not on the framework, so maybe didn’t have all the features mandated in the new contract. Some practices had been earlier adopters, made the investment then found that there was support to buy out of existing analogue contracts. Or course, anyone that has ever implemented new technology knows you can’t do it in a rush without good planning. Then after deployment comes the real fun – how to make it work for you. We saw this happen during the pandemic with the necessary but rushed roll out of online consultations.
Our team have been delivering workshops, listening to and improving auto attendant messages, optimising call flows, aligning with online service options, all to ensure fair access to services and an improved experience for patients. And then of course we threw in a Digital Journey Planner module around planning and optimising Telephony.
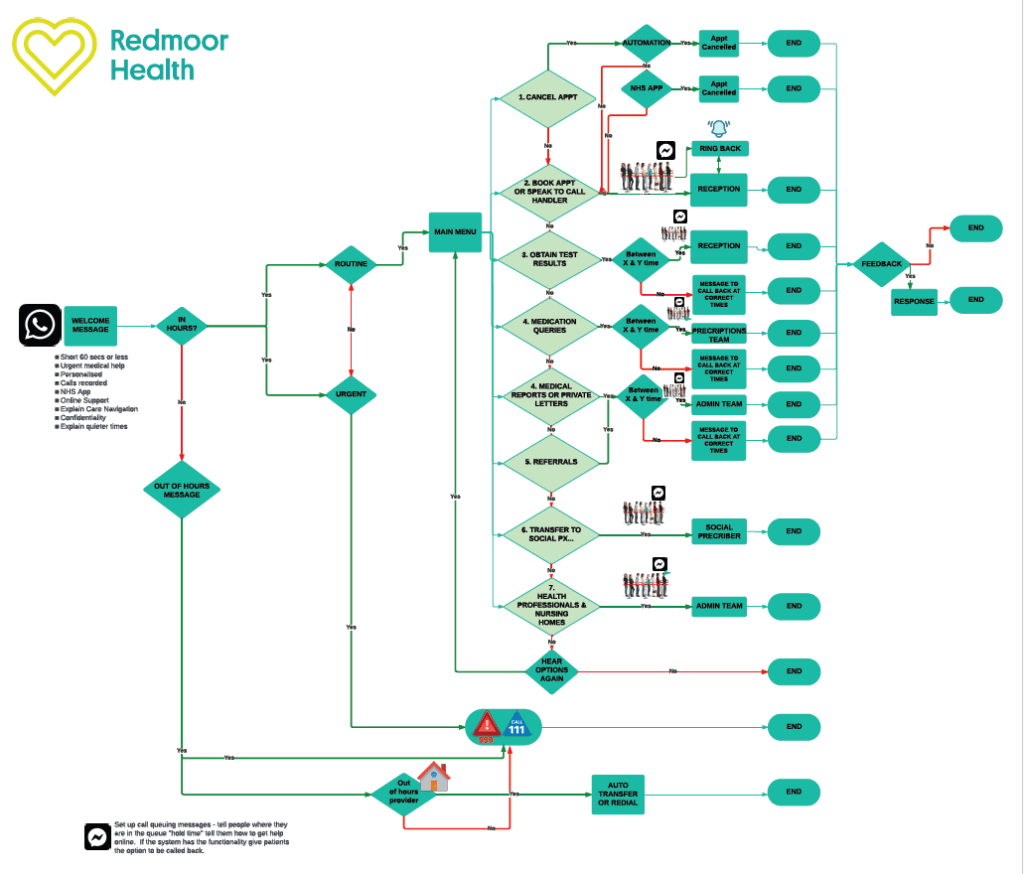
Example Call Flow options with routing out to alternative and online services
This is just a flavour of our support on offer to help the NHS at all levels in primary care to navigate the noise, help with the priorities, support the providers to deliver, optimising the solutions available. We hope you can come and see us at Best Practice at the end of the month, we’ll be at Stand D45 talking all things primary care improvement.
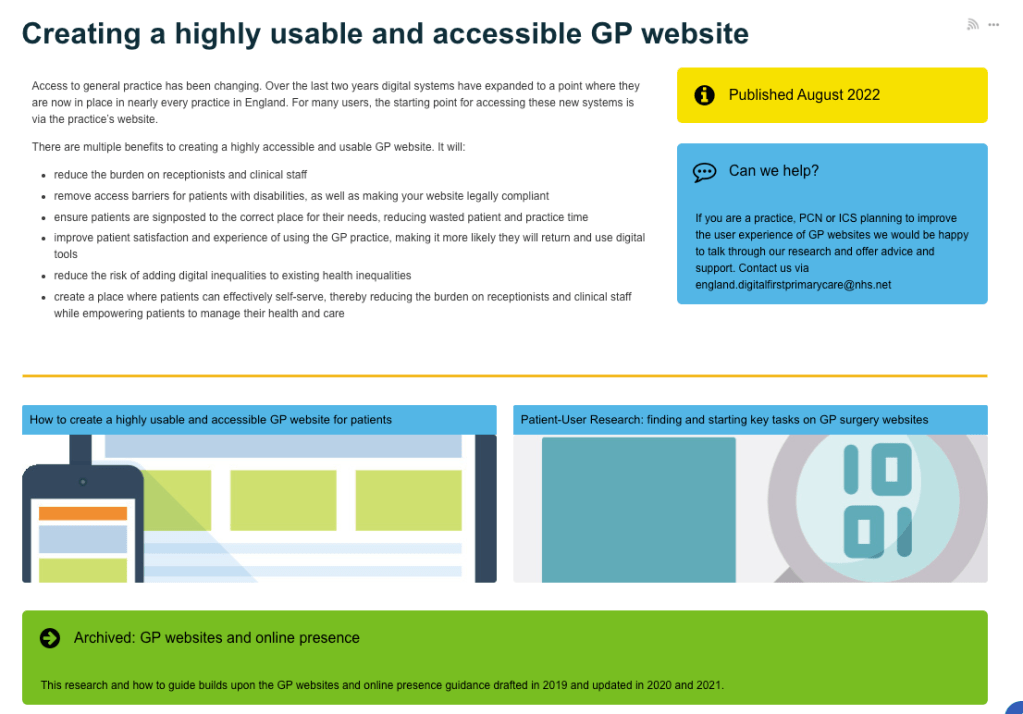
Future NHS page with the ‘creating a highly usable and accessible GP Website for patients’ guide, and ‘Patient-user research to support’
In the last few weeks there are some super updates to the guidance from NHS Digital and NHS England that will help GP practices to create inclusive content and usable websites. It should also make lives easier for people who need to use the ‘Digital front door’, aka GP practice websites.
You’ll realise that I have a bit of thing for GP websites. In my day job, I sit at the intersection between policy makers, NHS commissioners, specialists in inclusive and accessible research and service design, product suppliers and the people in practices who try and make sense of it all, to provide services to us as patients in the NHS. It’s a nice place to sit. I don’t need to be a specialist, I don’t need to have the technical know-how, and although I do know a fair bit about General Practice, service improvement and delivery, we all have experiences as patients that we can lean on and learn from. This guidance brings much of that knowledge into one place.
This is why the guides are so helpful….
GP Practices have a myriad of contract requirements to meet, in fact there are 10 pages of items listed in the ‘highly usable website guide’. Many of them are iterations of earlier contract requirements, it’s no wonder practice teams are confused – I’m confused by much of it too. The GP website supplier market is large, as is the online consultation market and each supplier clearly wants to do the best for their clients – the practices. But occasionally and possibly due to the market competition, these suppliers sometimes focus a bit too much on their own branding and product and not quite enough on the usability of their product, either from a General Practice team perspective or the intended end user, i.e. the patient. They may forget that their product needs to be connected to another NHS service and so needs to conform to the standards and style of the NHS brand, which is trusted and researched to reach as many people as possible. Often, the user is confused when they access information online and get diverted off to a supplier’s platform, or suddenly the page no longer looks like their GP practice or even an NHS service.
Home page from NHS Digital service manual showing the Standard for creating health content
Colours matter, language and content matters, the user’s journey matters, the technical layout matters. For the practice teams who have a million other things to do, simple ‘how to’ instructions and examples help enormously and these guides offer sample layouts with ‘things to include’ and just as importantly, things ‘not to include and say’.
Hilary Stephenson, Managing Director at Nexer Digital says,
‘It’s great to see the convergence of user centred design standards and technical platforms across the NHS and their vendor network. Sadly, in our work we have seen real issues with the core usability and accessibility of websites, consultation platforms and apps used for digital engagement. This feels like such a missed opportunity at a time where digital inclusion is vital for patients, their families and those delivering services under immense pressure. Anything that provides practical guidance, which is evidenced by user research and makes things more inclusive, from content design through to platform configuration, will improve the experience for patients, clinicians and administrative teams.’
Hilary Stephenson, Managing Director at Nexer Digital
Now the work starts….
There are over 6500 GP practices in England, just over 900 in Scotland, almost 400 in Wales and over 300 in Northern Ireland, each serving their average registered population of 9000 people. That’s a lot of people to reach to reduce the variation of experience for users and for practice teams who provide information. We have incorporated this guidance along with simple advice, hints and tips into an easy-to-use system called the Digital journey planner (DJP). The first module; Patient Communications deals with Websites, Social Media and Messaging, The second module; GP Online Services covers everything that practice teams need to know to provide a good online service and make that easy for patients to use. If you are getting ready for patients having full online access to their medical records later this year, it’s a must. Our next module, due for release at end of Sept will be Digital Inclusion.
Map showing location of practices in England using the Digital Journey Planner. Blue dots have Foundation access, green dots are practices with Enhanced support from Redmoor Health to embed digital service delivery. Aug 2022.
So far 10% of practices are using this system in England currently and we aim for 25% before the end of the year. At Redmoor Health we work with practice teams to help improve digital knowledge, skills, confidence and competence and offer support in terms of training, coaching, advice and share best practice resources that save practices time when searching for help. These guides are essential learning tools to embed in the DJP, so they are easy to find and stand alongside practical hints and tips when to use. Some areas have already commissioned Redmoor Health to carry out reviews across all their practice websites, just to get a feel for the scale of the problem and ideas how to help. Others have offered incentive schemes for practices to have the time and space to make the changes, so we anticipate this as a big opportunity to improve, standardise and simplify access to information.
The suppliers….
Good suppliers have been using these standards for some time and have already created NHS style guided website templates, that meet the accessibility and usability needs of users and practice teams. Others recognise that they need to encourage practices to move away from old legacy systems, personalised styles and ‘whizzy websites’ to be more consistent, and to simplify the user journey. I’m quite sure many more will now take on these recommendations following the detailed patient user research that informed the guide. I spoke to a few to get their views of the research and guidance.
Iatro Practice 365 have already produced a simple version and template for practice teams to know what to add to their website. Thomas Porteus said,
‘We’ve been behind the NHS Service Design Toolkit since we started, it’s been a pleasure to work with NHS teams openly and to be able to contribute our own code back to the project for the good of all NHS organisations. The guidance is a really great point of reference for practices wondering where to start, and what to avoid’
“As advocates for patient-friendly, accessible websites since we began working with GP surgeries in 2004, we warmly welcome this new evidence-based guidance from the NHS Digital First Primary Care team. Clearly focused on simplifying the patient journey, the guidance offers practical advice and tips for practices and commissioners aiming to improve patient experience, reduce digital inequalities and remove barriers to access for patients with disabilities.“
‘At Livi we welcome this new guidance from NHS England. Accessibility is not about sticking assistive technology onto the website. It is about building the website from the ground up to work with third-party assistive technology (e.g. screen readers). It is also about ensuring the website content is written in a way that is clear and understandable by the majority of users. By using the NHS Digital Service design system, Livi websites are NHS branded, optimising functionality and providing confidence for patients to engage with online GP services (as well as other locally commissioned services and third-party tools). We believe practices should have generic accessible content and definitions of local service providers to help patients manage their own care. This approach has allowed us to build a practice website platform that gives practices back more time to spend on patient care by:
nudging more patients to digital services and appropriate alternative NHS services,
reducing the time needed to manage and maintain the website
Dillon Sykes, NHS Partnerships Manager
To the commissioners – let’s do this together….
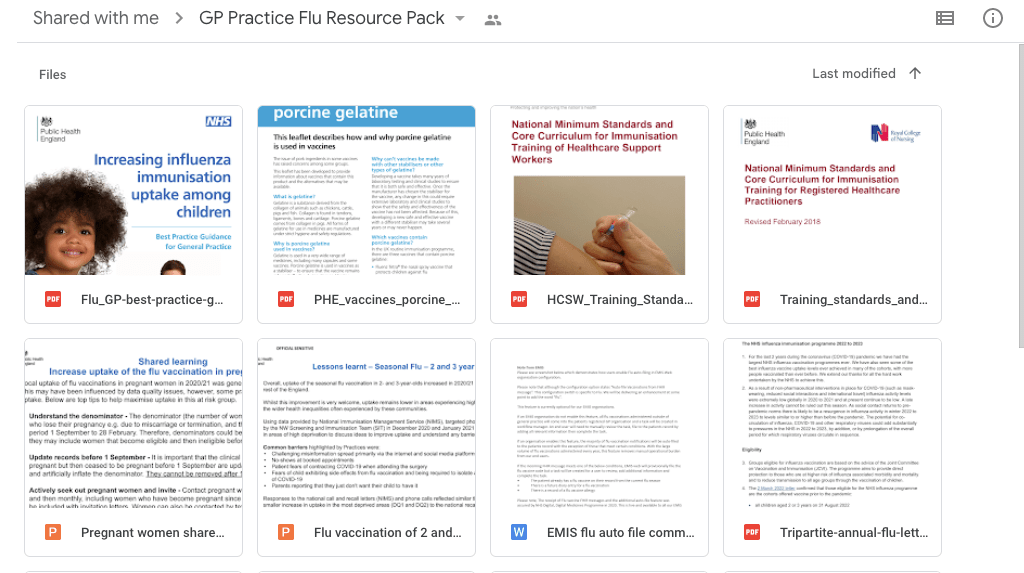
Most useful in the website guide is valuable information for NHS commissioning teams to help procure GP websites ‘at scale’ and to know what to ask of suppliers in terms of user testing. Perhaps now is the time to rethink the stance that ‘it’s a GMS requirement to have an online presence’. This must be the way forward to support local population communications and connecting the services at a local level for patients. It will support primary care network development and reduce the burden on individual practices to know and learn about website technicalities, so they can just focus on the message and how it is presented or accessed. As more services are delivered together, why would we expect each separate practice to upload its own content and service description? Surely this is done once by the local service provider? Let’s take a current example. Practices will all be delivering Flu and Covid boosters soon. They need one single page for who’s eligible, then the ability to edit and add what’s happening locally, so that people know how to book and where to go. Currently each website supplier may duplicate this, and some are good enough to offer a ‘Flu’ content page. NHS England have issued the criteria in a Specification. Public Health (UK Health Security Agency) have some promotional material, and poor practice managers will be trying to make sense of it all to tell their patients what is happening, whilst awaiting the final dates from vaccine suppliers and working out which members of the team can deliver. One forward thinking area has thankfully collated all of this information together for its member practices and wait for it…… shared it as a google drive document to 200+ practices via email!!! That’s my Friday job folks – to upload and create this years Flu page.
google drive document containing all of the information required for 2022/23 Flu campaign
Hopefully, you can see where I’m going with this. Do we really need 6500 individual digital front doors? I think not, but always open to be persuaded if you think the status quo is better.
I’ve had a nice experience today. I’ve had my ‘peer review’ with another practice manager, as part of the NHSE funded programme for Practice Manager Development. I volunteered to take part in the programme after a chat with the Lancashire and Cumbria LMCs, Programme Manager Sally Pern, when I was scouting around looking for things to do, rather than just (as if its ever just) being a practice manager. I’d contacted the LMC a couple of years ago to see if there was any funded support for PMs, as there was a system of support for GPs, but nothing for managers. I knew many of us were starting to creak with the increasing pressure and complexity of the job and were choosing to leave the system. As a Practice Manager, being the linchpin between GP Partners, Practice staff, Patients and external CCG/NHSE colleagues is sometimes a lonely and isolating place. The programme is intended to be both supportive for existing managers and developmental for deputies or aspiring practice managers.
Its all quite formal – it has to be to satisfy the paymasters that the money is being well spent. It also has to be ‘evaluated’ and ‘deliver outcomes’. First I had to fill in an application form, then have an interview to see if I was suitable and to identify what I could bring to the group in terms of experience. Its a bit strange being interviewed when its not for a ‘proper job’ and you know you’ve got a number of years experience doing the thing they are looking for. I still didn’t really know what was involved in the programme. After interview, I was invited to take part in two separate training courses; one to learn about the process and develop the paperwork and the second one to brush up my coaching and mentoring skills; both days expertly facilitated by Kevin Wyke, Liz Jones and Sally Pern. Kevin provided lots of useful hints and tools and demonstrated a coaching approach with Liz that I found refreshingly, (you get used to tip toeing around people as a manager these days) a lot more challenging than I felt I ever could be with a stranger, but it seemed to work. We are waiting to see that empty loft Liz.
As a group of reviewers, we quickly became comfortable and honestly shared our experiences and thoughts about the process and how the programme could help practice managers. Practicing our reviews helped us to realise that we have this knowledge and skillset, but coaching and supporting another manager may be very different from appraisals with practice staff. I am however, looking forward to my first reviews over the next few weeks.
Finally, before we start our reviews, we get chance to have a review ourselves to experience what its like. All so far so good.
Sally matched me with another Practice Manager from the programme, and today we both wondered aloud what criteria Sally uses to match people together. I had joked that I wouldn’t be an easy candidate, as I’m not sure I want to be a full time practice manager any longer and my reviewer had some trepidation too.
I was sent a guide and the ‘pre-review’ forms to fill in and had received the gentle nudge to return them before we met. When completing the forms at the weekend, I got a bit frustrated with the formatting – and a little sad that my offer to digitise the process hadn’t been taken up. Its crying out for a surveymonkey approach to make preparation, recording and reporting easier, but who knows, that idea might get adopted for the next round when the LMC team have to make sense of all of the cryptic responses. I also found it quite difficult to objectively answer questions about broad topics such as Governance, Sustainability, Management and leadership style, Relationships, Personal needs etc. I was beginning to wish I hadn’t volunteered and also reminded of why people find having and doing appraisals a bit of a pain.
The review is supposed to last 1.5 hrs, then we get an hour to write up an action plan. I cant imagine many reviews only taking 1.5 hrs as the time flew by and I think we could have spent longer. Managers don’t often get the chance to open up in a safe, confidential, non-competitive space, with someone who has total empathy and understanding of the role, environment, policy, powerplay, professionalism, personalities and pressures. And there is the real benefit of the programme. Not the ‘goals’ that I’ve identified, or the ‘actions’ that I’ve committed to, so that NHSE can be satisfied there is a ‘plan’ and that I’ll be ‘developed’ at the end of it. The part of significantly more value, was to be able to say to someone else, ‘what would you do?’ and to receive wisdom in a trustworthy, honest and pragmatic response, uninfluenced by any agenda, other than to support me in my role, in my career and in my life.
Thank you H, you did a great job.
PS, the comfy sofas, coffee, scone, jam and cream at Tebay services definitely created the right environment. I’d recommend it to anyone having a review.
It’s hard enough dealing with illness, worry and the pressure that results from this, without having a system which seems to be hindering rather than helping. I’ve been touched by an event where someone who cares for their son (he has a life changing, long term illness) is despairing because of the struggle to get access to his medical records to make sure he is cared for safely and receives the right medical treatment for his conditions.
I thought I would try and explain why some practices have not prioritised this area of work. That’s not to excuse them but more to give context to the problems. I hope this provides a broader understanding of the challenges so that if you too are struggling to get access to your records and need to have a conversation either with your practice or local CCG, this is easier because you know some of the background details.
Dr Hannan describes this as a Partnership of Trust and often a critical event like this triggers a huge swing in the opposite direction, hence their policy for openness and transparency. He is driven by this almost like a crusade and has been doing this for 13 years.
Unfortunately, the majority of GPs do not have either his reason or understanding of the benefits of providing full records access.
This post isn’t to debate the pros and cons, more to explain why it’s not as easy as presented. Most practices have only started in the last 2 years which have been an increasingly pressured time in General practice due to dwindling resources and increased demand. Our practice started to provide detailed online records access in 2015 following an evening training session with our patient group, staff and with Dr Hannan and yet according to the lastest NHS statistics, we still only have 33% of records access. I have been unable to spread this work across the practices in my area of Cumbria largely due to the chicken and egg situation; ‘patients don’t ask, so we don’t have to provide’ vs ‘patients don’t know what to ask for, or when they do ask, its too hard to do’ for the practice. I also support our local group of PPGs and help to raise awareness about the benefits of records access and I’m often frowned at by my PM colleagues, who are finding it hard enough to do the day job with multiple complex priorities and change.
We are dealing with a society where increased litigation is creating more fear in clinicians than ever before, ramped up by risk aversion and caution in the medical indemnity and professional bodies such as RCGP
The guidelines we have to follow and assurances we have to give to regulators (CQC) are confusing and completely at odds with patient experience and NHS policy directive ie our GMS contract See Section 3.
Pulse, like many other organisations provide both detailed and summary guidelines to address the new GDPR regulations but interpretation is varied across practices, some provide the absolute contract minimum records access, others have increased their provision rather than deal with Subject Access Requests.i
I know there are really good General Practices, with Outstanding recommendations from CQC, who still only have 0.27% for their Detailed Care Record Access.
As a member of a patient group, I have asked my practice to enable some of this functionality, but have stopped asking as I’m aware that I could be perceived as a nuisance and that this may affect our relationship. So I appreciate the experience from both sides of the divide.
If you are interested to see how your local practice compare, here is the latest data so you can find your CCG and practice and see where they benchmark.
Many of you will know that General practice income is reducing year on year and expenditure increasing. The Independent contractor business model means that any additional unfunded work comes directly from the bottom line of GP Partners income. If Partners have a choice to pay locums to keep the service going, rather than spend this on clinical and admin time to carry out the data checking required to ensure the records are accurate, readable, viewable and cleansed (I mean redacting any 3rd party information which is required by law), then they will spend their money on the locum every time so that patients get seen. It’s a continual balancing act between providing access and shifting to new ways of working.
GDPR has increased this anxiety and whilst from a patient perspective, the regulation is a good thing i.e we should know what’s in our records, this has created a huge amount of work in practice. Software to help carry out this process is available such as iGPR but at a cost to the Practice or the CCG and is only recently developed. Initial feedback is good, but their earlier versions of their insurance reports were clunky so many practices were put off by this.
Think back to the days when your GP wrote in Lloyd George paper notes, probably in medical shorthand to describe what your symptoms were. Many of these old records are illegible, some contain inappropriate comments as societal norms and subsequent language has changed. These were always the ‘GPs notes’, not the patient’s – but now thats changed, even if the content in the notes is the same.
Each time a patient moves from one practice to another, your new GP then becomes the data controller for someone else’s data entries. Would you be happy with this responsibility and be willing to share without checking the historical records? Until recently, none of this was taught in Medical School and I suspect its still skipped over. Our practice teach medical students – this topic is always on our training schedule – even if the Student tells me they want to be a surgeon.
Roll forward to today when people are requesting 10-30 years of this history to be viewable and I think you can appreciate the workload to share this in a presentable way.
Another feature of GDPR (in addition to the increased workload and anxiety) is the removal of the ability to charge for the work. Hence, some practices suggesting to all patients that online access is the answer and then realising the workload to tidy the records is no less onerous than printing them. Yet Practices still have to put in place mechanisms to ensure that records are continually checked for external 3rd party content and protect this information from disclosure.
I’m not aware that NHSE have provided any direct resource linked to the volume of this work to practices since 2012, when they funded a Direct Enhanced service for online services for a short period. This work is now incorporated as a GMS contract requirement for online services, with a ‘stretch target’ for further adoption. The current figures mainly reflect use of transactional services (online appointments and medication requesting) to present the story of ‘14million users’, so this satisfies the DH & Secretary of State’s headlines of success, but provide little support in terms of detailed care records access. NHSE Patient Online team have reorganised as the ‘Empower the Patient team’ and whilst offer presentations and promotional materials to support practices, they do not have any budget for deployment or direct training at a practice level.
CCGs are responsible for the Infrastructure to support General Practice in terms of IT and local Training capability and capacity varies from area to area, so unless the Practice team has some understanding of what the patient can see through the various record viewers, then they wont understand the consequences of scanning correspondence, without details being attached to the images. Correspondence may have scanned historically before this became a priority, hence many online records have no valid descriptions on the attachments. Practice priority is to get the correspondence into the records asap so that if a patient comes into the surgery, the clinician can view the letters or act on the information contained therein. Bulk adding of correspondence is a common task, followed by summarising of ‘read coded’ information and if a patient has a large record, then often the GP2GP (thats the electronic system for transferring the electronic record) fails. So someone has to painstakingly read every piece of correspondence to glean the pertinent details and manually code this information. There are add on software products that can help, but stable infrastructure is required or else this adds further risk if documents cant be accessed by the clinician in the consulting room.
In our practice we have 3 years worth of scanned images from 2006-09 that are unable to be converted into a viewable format. That was due to the scanning system configuration at the time and long before records access was even considered. Our CCG paid for the remainder of our historical scanned images to be converted to a readable format. Many practices have to fund this cost themselves.
As Ingrid Brindle regularly points out, complex patients or their carers often have the best knowledge of their history – she says ‘it’s their life’s work’ and patients can be a great support to help practices correct any inaccuracies. Patients can help by highlighting all of the pertinent information and checking with their practice that this is:
A. Read coded
B. In a format that is shareable across the health organisations in their area
C. Visible through whatever records viewer a patient chooses to use.
The introduction of Snomed might make it easier for hospital coding to be automatically transferred into GP records but this has been in the pipeline for many years, although expected later this year.
Sorry this was a long post, but as you can hopefully see, this isn’t an easy or quick fix and it shouldn’t be left to individual practices to resolve. NHS Digital seem to be focussing on front end entry to the NHS through apps and also single identity authentication to remove the need for multiple passwords and sign ins. They are currently working with existing market providers like Evergreen Life and Patient Access for the records viewing element but its not clear yet how this will impact on records access at a practice level.
Alongside this, CCGs and clinical system/Electronic health record providers are focussing on large scale inter-organisation data sharing, but not direct sharing with the patients. It will be interesting to see if the launch of the NHS app for accessing all services increases the requests from patients for records access online and how this will be resourced.
I’m sort of messing about a bit, trying something new and then seeking a bit of feedback (I hate that bit already), maybe just a bit of a reaction to see what this blog might generate.
Glenys has said a couple of times – ‘why don’t you write a book’? This is usually when I’m sharing a story of an event because sometimes, there is a back story to a headline which would make your toes curl. But that’s maybe for another blog.
I suppose the quick answer is, I rarely sit down long enough to think through what I want to share. Although, I am a sharer by nature and like connecting people who have shared interests to help them make their things happen.
So this week during a coaching session, Claire encouraged me, in a very gentle way, to start blogging. Its raining outside (finally), so I’ve registered with WordPress and I hope to use it to share further experiences through ‘What Lisa did next….’
Earlier this year, I blagged a place on the Innovation Agency’s Coaching Academy for Spread and Adoption programme. They are recruiting again and I’d recommend it to anyone with an idea or innovation that they want to share. I say blagged because I’m actually in the North East AHSN patch but I couldn’t see this course in my area, so felt it was worth an application. I was about to take a sabbatical and test if I could start working in other areas, both geographically and in other sectors, as I was ready to change in career direction.
I hoped the programme would help with one of my regular challenges at work; trying to spread a message about using digital tools, techniques and services to a large majority of people who don’t quite get what I’m talking about. I know that sounds vague but all I’m trying to achieve is to bring the everyday technology and experience of our life outside of work into General Practice, where I’ve worked as a Practice Manager for 8 years. I’m talking about the sorts of things we take for granted; we bank and book train tickets, holidays and events online, we chat and network using Social Media, we use ‘phones, tablets, gadgets and devices, software and apps to carry out these activities, yet in the parts of the NHS if you talk about using this type of ‘Digital’ stuff to deliver services or make workload efficient, many people glaze over and then often get confused with IT, Tech, hardware and infrastruture and geekiness – or at least it seems that way in General Practice and in many areas of the NHS in Cumbria. That’s perhaps understandable given the pressures in General practice where its hard to innovate when practices are struggling to keep going. I said to a CCIO recently, ‘sometimes, I feel like an alien amongst my Practice Manager colleagues’, they replied, ‘that’s because you are like one, to them’. Yet, I know this isn’t the case everywhere and I’ve been fortunate enough to work with the Healthier Lancashire and South Cumbria Digital Workstream on the Primary Care Digital Exemplar Programme. This has provided me with the space to try to develop my message and also to realise that if the context and environment is ready for this message, its heard and spread with enthusiasm. I am meeting like minded General Practice colleagues who are ready to adopt these new ways of working.
By the way, I’m none of the above – neither alien, technically gifted or geeky and I most definitely suffer with imposter syndrome when working alongside truly talented individuals who know about User Experience & Digital Design, Technical architecture and infrastructure and System configuration.
But I do know a fair bit about introducing new ways of working, going at the pace that people can cope with when introducing change, about the need to explain what we hope to achieve and why, also about how to help people learn to use something they feel a bit unsure of. And I mean both NHS employees and people who use our services.
So that last paragraph helps me a little to understand myself a little better. I think that I’m able to look for the stuff thats out there, see the opportunity for its use in improvement, maybe interpret the strategy and then link it to delivery, whilst understanding the pressures and level of competence in general practice. I’ve no idea what job title you would give to that role. Any suggestions? Feedback and reaction most welcome.



















 wondered aloud what criteria Sally uses to match people together. I had joked that I wouldn’t be an easy candidate, as I’m not sure I want to be a full time practice manager any longer and my reviewer had some trepidation too.
wondered aloud what criteria Sally uses to match people together. I had joked that I wouldn’t be an easy candidate, as I’m not sure I want to be a full time practice manager any longer and my reviewer had some trepidation too. s crying out for a
s crying out for a 


 but their earlier versions of their insurance reports were clunky so many practices were put off by this.
but their earlier versions of their insurance reports were clunky so many practices were put off by this.

